The intersection of healthcare and immigration policy is found in the halls of hospitals and clinics across America, where increasing numbers of International Medical Graduates (IMGs) are filling in for doctors who won’t return, and state governments are doing their best to usher IMGs into practice where they’re sorely needed.
Help (Badly) Wanted: Foreign Doctors Apply Within
In 2023, Tennessee became the first U.S. state to drop residency requirements for some IMGs,1 giving them a new pathway to permanent licensure. Following Tennessee’s (somewhat surprising) lead, at least 15 states have introduced legislation to create streamlined pathways to medical practice for IMGs, with both Republican and Democrats contributing.2
During the 2025 state legislative sessions, over 20 bills have been introduced that would expand opportunities for IMGs to support America’s healthcare workforce needs. These range from allowing qualified DACA recipients to apply for licensure in New York to removing redundant training requirements in Montana.3
Some state legislation is more focused in scope. For example, in Illinois, IMGs must not only be legally able to work in the U.S., but are also mandated to work in medically underserved areas.
Perhaps most shockingly, in 2024 Governor Ron DeSantis of Florida signed the “Live Healthy” initiative to allow IMGs to bypass residency requirements if they have equivalent training experience. But then, the largest population of IMGs is in geriatric medicine, where they make up more than half of the physician population. And, well, it’s Florida.
Already at their shift
For that matter, according to the American Medical Association, a full 25% of licensed U.S. physicians are IMGs,4 with the largest number coming from India, followed by the Caribbean, Pakistan, the Philippines, and Mexico.
This is where the cognitive dissonance comes in– or at least, it should.
The new administration’s condemnation of everything related to equity and diversity, coupled with its rabid pursuit of an America free from immigrants, is simply incompatible with this reality. The reality is that massive numbers of the country’s doctors come from foreign countries, and are supported by legislation and advocacy work focusing on combatting racial and ethnic disparities.56
The AMA’s International Medical Graduate (IMG) Toolkit, in its section on “Academic opportunities and scope of practice,” acknowledges the fact that IMGs will face discrimination, but encourages them to press forward:
IMG physicians face several barriers in their goals and aspirations towards a career in academic medicine. . . Systematic exclusion is also a reason leading to discrepancies in leadership positions and promotions among IMG physicians. Despite challenges, IMG physicians are encouraged to choose an academic career as diversity is a strong determinant of innovation in medicine.”7
Those words “strong determinant” stick out to me, having written so much about social determinants of health.8910
A strong determinant doesn’t make a result inevitable, but rather highly likely. “You have something to contribute,” this guidance says, “So don’t give up in the face of discrimination. Keep trying, because we need you.”
I wonder if America is aware of how much we need IMGs, and how opponents of “DEI” and immigration reconcile their views with this reality.
Wait, actually I don’t. The reality itself is what matters– it’s where IMG physicians can, and do, make an enormous difference.
The language used to justify policy is…fraught. Every new program is a triumph, as is every cut to an existing one. Every new rule is a sea change, and every executive order a roadmap to utopia. These flowery-but-decisive statements come from all politicians, pointing in all directions, and they always have.
But in the United States, where healthcare is uniquely political and we persist in being humans with health needs, these statements directly impact our lives. We must pay attention. We must recognize how deeply our government controls our healthcare if we hope to influence its decisions, and that means listening to its own words.
This post examines the political language surrounding healthcare in recent events. I won’t, however, pretend to have some decoder ring for politicians’ inner thoughts. I don’t need one—their intentions are right there in plain language. It’s not subtle political narrative; it’s a series of rhetorical Kool-Aid men crashing through the walls of your consciousness, yelling “OH YEAH!” every time. Every. Single. Time.
“Lowering costs”
For example, the Trump administration recently issued an executive order “to empower patients with clear, accurate, and actionable healthcare pricing information.”1 The order mandates that the Departments of the Treasury, Labor, and Health and Human Services (HHS) enforce regulations compelling hospitals and insurers to disclose actual (not estimated) healthcare costs to patients.
The goal is “lowering costs for American families.” “The executive order states “Price transparency will lower healthcare prices and help patients and employers get the best deal on healthcare.”2
Enforcement of these regulations falls to the Centers for Medicaid and Medicare Services (CMS) within HHS, using three main avenues for monitoring compliance. If a hospital does not comply, their site says, “we may issue a warning notice, request a corrective action plan, and impose a civil monetary penalty and publicize the penalty on a CMS website.”3
To be clear, I think healthcare pricing transparency is a great idea.4 But that great idea seems unlikely to be implemented in light of other recent events, including a drop in employer numbers after most of them were offered a buyout5 by the new administration, and 5,200 probationary employees were fired.6
Perhaps that administration has determined that the CMS will have extra spare time and funding to check compliance as it abandons a foundational and essential goal on the basis of sheer ideology– but we’ll get to that below.
Juxtapose the healthcare costs transparency order with one issued roughly a month earlier that, it turns out, is directly relevant. On January 20, Donald Trump mandated that the federal government should:7
Terminate, to the maximum extent allowed by law . . . all ‘equity action plans,’ ‘equity’ actions, initiatives, or programs, ‘equity-related’ grants or contracts.”
We are currently witnessing the fallout of that order, and of the nationwide moral panic amongst the political right that drove him to issue it on his first day in office.
“Eq*ity”
But what does this allegedly dirty word even mean, in the context of healthcare?
The goal of achieving health equity was articulated by the previous administrator of the CMS, Chiquita Brooks LaSure, in the CMS FY2025 performance plan:8
As the Nation’s largest administrator of health benefit programs, CMS is uniquely positioned to accelerate initiatives that advance the Secretary’s commitment to enhance mental health services, transform pandemic preparedness capabilities, and advance health care quality. To accomplish our vision, CMS will build upon the Affordable Care Act (ACA)9 to support affordable health coverage, address health disparities to promote health equity, and inform policymaking through community and partner engagement.
And (for now, at least) the CMS.gov website defines health equity in this way:
The attainment of the highest level of health for all people, where everyone has a fair and just opportunity to attain their optimal health regardless of race, ethnicity, sexual orientation, gender identity, socioeconomic status, geography, preferred language, or other factor that affect access to care and health outcomes.10
How long has the concept of health equity been around? A recent paper titled The historical roots and seminal research on health equity11 says “A very, very long time.”
Research on health equity experienced three important historical stages: origins (1800–1965), formative (1966–1991) and development and expansion (1991–2018). The ideology of health equity was endorsed by the international society through the World Health Organization (1946) declaration based on the foundational works of Chadwick (1842), Engels (1945), Durkheim (1897) and Du Bois (1899).
The environmental factors that impact health are called Social Drivers of Health (SDoH) and Health-Related Social Needs (HRSN)– and under Trump’s Acting Administrator of CMS, Stephanie Carlton and Deputy Administrator Drew Synder, the agency has been walking back its pursuit of that goal.
An “ideological crusade”
As of March 4, The Centers for Medicare & Medicaid Services (CMS) has pulled information on health equity for the Medicaid and Children’s Health Insurance Program (CHIP) through Section 1115 waivers,12 a move that former chief medical officer for the Medicaid program at CMS Andrey Ostrovsky, M.S. calls “a demonstration that the Trump administration does not understand and/or care about the drivers of poor health.” “Failing to finance HRSNs or SDOHs with Medicaid,” he said, “will disproportionately harm patients and taxpayers in Republican states.”13
Senator Ron Wyden of Oregon was more blunt, accusing newly-minted Secretary of HHS Robert Kennedy of an “ideological crusade against Medicaid.”14
Services that CMS has provided coverage for, based on HRSN data, include home accessibility modifications like handrails and wheelchair accessibility ramps, transportation vouchers, rent or utility assistance, and care coordination– helping individuals manage their care plans.
What’s the justification for the change? A memo15 by Snyder states:
To support implementation of coverage of certain services and supports to address “health-related social needs” (HRSN) in State Medicaid programs and Children’s Health Insurance Programs (CHIP), the Center for Medicaid and CHIP Services (CMCS) issued two Center Informational Bulletins (CIBs). The first. . . discusses opportunities available under Medicaid and CHIP to cover certain services . . .that purport to address HRSN. . . To evaluate policy options consistent with Medicaid and CHIP program requirements and objectives, CMS is rescinding the November 2023 and December 2024 CIBs.
“Purport”
In other words…no justification. Not even an attempt– just “We no longer care about this. Because, that’s why.”
But that little word “purport” in there fascinates me. Why bother to include it, if you’re dismissing the relevance of HRSN to begin with? Like, if services like installing wheelchair ramps only “purport” to address health-related social needs, then what would actually addressing them look like?
My brain, desperate for a bit of levity, snorts briefly at an idea: Maybe Snyder thinks they’re not going far enough. Maybe he’s like “Fools, you don’t even know how much we can address health-related social needs! Watch me cook!” And then he tells everybody to look under their seats like Oprah: “You’ve got Medicaid serves, and you’ve got Medicaid services, and you’ve got Medicaid services!”
Sadly unlikely, but I sure wouldn’t mind living in that universe.
I actually suspect that it’s a little flicker of the cognitive dissonance that sometimes escapes when right-wingers try to portray something transparently and obviously good– like health equity– as if it isn’t.
Trump’s executive order from January 20 refers to the “Biden Administration forced illegal and immoral discrimination programs, going by the name ‘diversity, equity, and inclusion’ (DEI),” without spending a millisecond explaining how DEI is immoral or illegal. Why? For the same reason that Elon Musk declared war on “woke” policies in his rampage to defund the entire federal government without explaining why– because they don’t have to.16
“Make America Healthy Again”
Let’s go back to CHIP for a moment. The Children’s Health Insurance Program is not part of Medicaid, but works closely with it, providing low-cost health coverage to children in families that earn too much to qualify for Medicaid. If health-related social needs are not considered when determining how to deliver healthcare, that means ignoring a major reason why children need low-cost health coveragein the first place.
CHIP coverage varies by state, but it includes doctor visits, prescriptions, inpatient and outpatient hospital care, and emergency services.17
Why do kids need all of those? Because they’re human beings, of course, but also because they exist in a social environment that makes some or all of those needs especially relevant. Some examples:
Housing Instability: Children in unstable housing have higher rates of asthma due to exposure to mold, pests, and poor ventilation.
Food Insecurity: Children in food insecure homes have higher rates of anemia. Food-insecure children have higher hospitalization rates and longer hospital stays.
Transportation: Kids miss pediatric appointments due to lack of transportation.
Health literacy gaps make parents more vulnerable to vaccine misinformation
An assessment of the latest CDC National Immunization Survey data found that more than one-third of U.S. children between the ages of 19 and 35 months were not following the recommended early childhood immunization schedule. Furthermore, a 2019 national survey found that approximately 1 in 4 parents reported serious concerns towards vaccinating their children. Vaccine hesitancy is now associated with a decrease in vaccine coverage and an increase in vaccine-preventable disease outbreaks and epidemics in the United States.
Oh, and there’s that measles outbreak in West Texas:19
Texas health department data shows the vast majority of cases are among people younger than 18: 39 infections are in kids younger than 4 and 62 are in kids 5-17 years old. Eighteen adults have measles and five cases are “pending” an age determination. . . Most kids will recover from the measles if they get it, but infection can lead to dangerous complications like pneumonia, blindness, brain swelling and death.
That’s from the AP, who took the time to directly refute our new Secretary of Health and Humane Services:
The MMR vaccine is safe and highly effective in preventing measles infection and severe cases of the disease. . .
Before the vaccine was introduced in 1963, the U.S. saw some 3 million to 4 million cases per year. Now, it’s usually fewer than 200 in a normal year.
There is no link between the vaccine and autism, despite a now-discredited study and health disinformation.
“But I do have reservations with your past on vaccines”
And yet Robert Kennedy, who made a promise to Sen. Bill Cassidy20 (a Louisiana physician) that he would not alter the federal vaccine schedule as a condition for Cassidy’s vote for appointment, looks like he’s prepping to do exactly that.21
Speaking for the first time to thousands of U.S. Health and Human Services agency employees, he vowed to investigate the childhood vaccine schedule that prevents measles, polio and other dangerous diseases.
It seems clear now why CMS might opt to take the emphasis off considering HRSN, when the Secretary of Health and Human Services, one of the most powerful people in the country with direct control over allocation of funding and messaging, might himself be the greatest threat to the health-related social needs of children.
“Nothing is going to be off limits”
That’s what he said regarding the scope of his so-called investigation, including inquiries into the effects of pesticides, food additives, microplastics, antidepressants, and “electromagnetic waves emitted by cellphones and microwaves.”
But in reality, he’s referring to children’s’ lives. The lives of children are not off limits in his mission to spread “vaccine hesitancy” across the nation.
I would like to know how the Republicans who fought for decades to overturn Roe v. Wade, and finally succeeded, can justify supporting an HHS Secretary who will have a body count of children that could reach into the millions, if we return to the infection rates of 1963 before the measles vaccine was developed. Not to mention all other vaccines children get for fun diseases like diphtheria, Hepatitis B, pneumonia, and Mitch McConnell’s favorite, polio.22
But hey, at least the fortunate children of parents who want them to be vaccinated, but who can’t afford it, can still get vaccinated through the Vaccines for Children program.23
Yes, the legislation that Republicans tried 70 times to “repeal and replace,” and that Trump still claims he has a “concept of an idea” for what should replace it. ↩︎
And given that these slogans-turned-smears all originated in helping people of colors other than white, it doesn’t take a space rocket surgeon to discern the true reasons for failing to elaborate. ↩︎
One of my first-year classes in college was History of Theater, in which I learned how the Greeks built amphitheaters into hillsides, carving out a semicircle of seating for the audience around the stage to maximize. The scenery for a play completes the circle, just as it does for any show in an amphitheater today. It’s the structure providing the necessary atmosphere for the experience.
Imagine sitting in such a theater, watching Euripides’ Helen, and seeing the demigods Castor and Polydeuces (Helen’s pissed off brothers) descend into the scene by a wooden crane—a mechane — whereupon they put an end to all of this murderous nonsense, and everybody lives happily ever after. It’s a literal top-down solution.
That’s where the expression deus ex machina, or “god from the machine,” comes from. And it became used, and mocked, throughout the world of fiction as a plot device providing a too-convenient, cheap ending to a story.
But my mind just keeps going back to that silly crane. It used to dangle a man dressed as a god before the audience, but these days he’d more likely be a techbro holding a smartphone, probably talking about the wonders of AI.
That’s on my mind today because in this post, I’m about to dangle a hypothetical mobile app in front of my audience– you. I illustrate our country’s mess of a healthcare system, and perhaps even reckon with it. This play isn’t ending any time soon, and we need to find a role in it (else one is chosen for us).
Healthcare data and analytics company Arcadia recently launched its own talk show, Spicy Takes, to discuss “hot perspectives in healthcare” while sampling—you guessed it—spicy food. The first episode placed President and CEO Michael Meucci in conversation with Chief Product and Technology Officer Nick Stepro and Chief Medical Officer Dr. Kate Behan.
I watched it while reading about their SDoH (social determinants of health) package, which promises to justify the time and expense required of providers to consistently record SDoH data by creating registries mapping that data with diagnostic codes, for use in proactively identifying patients at risk and connecting them to resources. While looking over the tear sheet, I heard Meucci say this:
I think that this is such a great platform for digital health as we start to think about how do you democratize access. Because if a patient is concerned that they’re not going to get the right treatment because of the color of their skin or the community they live in, the smartphone is a great equalizer. We talk about what’s changed for the last 10 years—that, to me is the biggest thing, the fact that you can pull out your phone and get connected with a doctor in 15 minutes.
“To your point, Stepro replied, “all of the technology and all of the access to healthcare in the world doesn’t change the fact that the single worst diagnosis you can have as a patient is being poor. You can’t address that with a healthcare institution. We can measure that poor people have lower outcomes but ultimately, we need to find and attack the problem of homelessness and poverty because you can’t just solve that in a clinic or with a smartphone.
I stopped reading and played that section of the show again. Meucci didn’t say that the healthcare industry can solve poverty with smartphones; he said we could democratize healthcare access. If that’s a spicy take then you can call me Spice Girl, because that’s my healthcare platform now. But I suppose coming from someone like him, that’s practically revolutionary.
And he’s right. As a country, America is primed for solutions like that: over 91% of Americans have smartphones. Even households without broadband hang on to their smartphones, because of course they would—it’s a tiny computer that can do more than any of us ever seem to realize, or ever will.
Democracy—another word with ancient Greek origins– literally means “power in the hands of the people.” What would it even look like to do that with a smartphone?
Let’s do a thought experiment to find out.
Time to design a smartphone app.
Imagine that in the beginning of The Legend of Navigating the American Healthcare System, our player character is given their first smartphone.
On that phone there’s an app installed (that I’ve just invented) called HACK: Health Agency, Care, and Knowledge.
Health – A full, patient-owned medical history
Agency – Control over your care, your records, your choices
Care – The power to find, compare, and advocate for treatment
Knowledge – Because to be informed is to be empowered
Does your vision of this app include it conferring access to all of an individual’s health records, stored securely but also accessible in their entirety at any time? If so, you’ve envisioned something better than what existing patient portal apps currently provide.
So yes, let’s absolutely start there, if we’re designing an app that democratizes healthcare in America.
And remember that democracy means that the power is in the hands of the people—not the “patients.”
Problem: we’re not in the driver’s seat.
Social Drivers of Health (SDoH) is the category of data on an EHR encompassing the non-medical factors affecting an individual’s health. In other words, your life, from the hospital where you were born (if you were born in a hospital) to the destination of your organs when you die.
They’ve been called the social determinants of health, but the word “determinant” suggests finality, immutability—that there’s nothing you (or anyone) can do about it. A driver, on the other hand, suggests that while the deck may be stacked against you, things could always change.
How easily could you could do that? *shrug* It depends, but we can safely say that “resident of the United States” is not an easy “driver” to change. We’re driving that road whether we want to or not.
And I hate to break it to you, but we live in a hostile health environment.
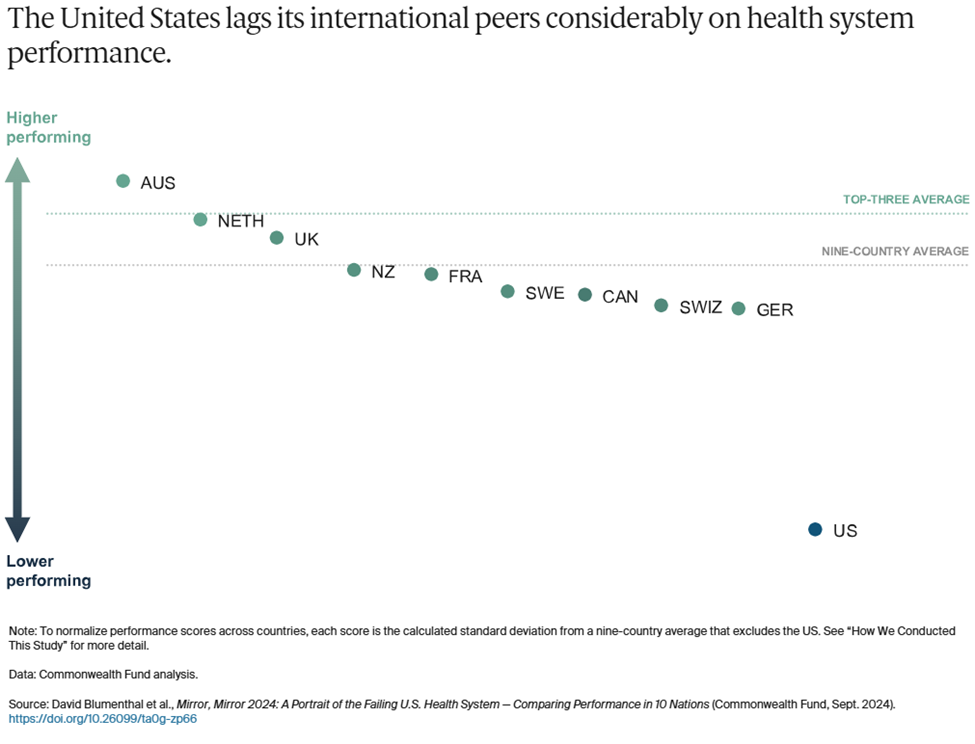
A 2024 study titled Mirror, Mirror 2024: A Portrait of the Failing U.S. Health System was conducted by The Commonwealth Fund to understand why America is doing so poorly by comparison—that is, going beyond the factor that rhymes with “schmooniversal schmealthcare.” The categories they used are:
Access to Care
Administrative Efficiency
Equity
Care Process
Health Outcomes
In all but one of those categories, America comes in dead last or next to last.
To summarize the report, it found that Americans spend more on healthcare as a percentage of GDP to receive lower healthcare system performance than other countries. It faces the most barriers to accessing and affording healthcare. Its physicians and patients are most likely to face hurdles related to insurance rules, billing disputes, and reporting requirements. Equity in healthcare access and experience is low. And we live the shortest lives and have the most avoidable deaths. All by a longshot. USA! USA!
The one exception in these categories is Care Process, where we came in second. Their comments:
Care process looks at whether the care that is delivered includes features and attributes that most experts around the world consider to be essential to high-quality care. The elements of this domain are prevention, safety, coordination, patient engagement, and sensitivity to patient preferences.
I interpret this result as an indication that some version of enabling people to take charge of their own healthcare is key to accessing that care in spite of all other factors. It could even, possibly, raise America in those other categories where we’re currently ranking dead last!
Okay, probably not, but it could definitely help us face the hostile health environment in which we currently exist:
Misinformation is everywhere.
We live in an era where vaccine misinformation spreads faster than the viruses they prevent, leading to the resurgence of eradicated diseases, overwhelmed hospitals, and preventable deaths fueled by fear rather than science.
We live in an era where people google their symptoms and often reach the worst, scariest conclusions that inadvertently contribute to their paranoia, where “doing their research” on healthcare can lead to being convinced of conspiracy theories and pseudoscience.
We live in an era where the president of the United States once advocated for injecting disinfectant as a means of staving off Covid, and in his next term has appointed a raw-milk-drinking anti-vaxxer as Secretary of the Department of Health and Human Services.
We live in an era where social media influencers with no medical expertise gain massive followings by promoting unproven “natural cures,” convincing people to reject evidence-based treatments in favor of detox teas, essential oils, and dangerous fad diets
We can’t afford anything.
We live in an era where Cost-Related Nonadherence (CRN) is the primary reason for medical nonadherence (failure of patients to take their medication as prescribed due to cost) in some cases forced to choose between “treating and eating.”
We live in an era where the term “dual ineligibility” refers to the status of undocumented immigrants in the U.S. who qualify for both Medicaid and Medicare, but are unable to access either one.
We live in an era where medical debt is the leading cause of personal bankruptcy, where a single hospital visit can trap families in a cycle of financial ruin, and where crowdfunding platforms have become a substitute for a functioning healthcare system.
We live in an era where rural hospitals are closing at alarming rates, leaving entire communities without nearby emergency care, prenatal services, or even a local doctor, forcing low-income patients to travel hours for basic medical attention they still might not be able to afford.
Neighbors hate and fear their neighbors.
We live in an era where in transgender healthcare, patients frequently encounter providers who lack adequate knowledge of gender-affirming care or hold prejudiced views that hinder appropriate treatment.
We live in an era where in reproductive healthcare, political and ideological barriers, including misinformation and ignorance, stand in the way of basic, safe medical care.
We live in an area where Black patients are more likely to have their pain underestimated and undertreated, leading to worse health outcomes.
We live in an era where in disability healthcare, patients struggle to have their pain, symptoms, and autonomy taken seriously, with providers sometimes dismissing concerns as psychological or unavoidable aspects of their condition rather than treatable medical issues.
We live in an era where in chronic illness care, patients—especially women—are more likely to be dismissed as exaggerating their symptoms, leading to years-long delays in diagnosis for conditions such as endometriosis, fibromyalgia, and autoimmune diseases.
We live in an era where in elder care, aging patients often have their autonomy disregarded, with medical decisions made on their behalf without full consent, reinforcing the notion that age diminishes a person’s right to control their own body and treatment.
We live in an era where fat patients are often told to lose weight as the solution to every health issue, leading to delayed diagnoses and overlooked conditions that have nothing to do with body size.
We live in an era where for immigrants, language barriers, lack of documentation, and fear of discrimination or legal consequences discourage people from seeking medical care, exacerbating preventable conditions.
But remember: “they” are us, and we all deserve better.
If you’re still thinking about this in terms of how we can help them by this point, stop it. That’s “patient engagement” speak, and our identify is not “patient.”
Our identity is “person,” i.e. member of the human species, class Mammalia, spending every second of life alive, for 100% of the time (until we’re not), thus making our health, and healthcare a relevant part of our lives 100% of the time. Yes, even for doctors.
We all should get a remote control.
A note ondignity: Meucci mentioned not getting the “right” treatment based on the color of your skin or the community you come from, suggesting that a smartphone could be “a great equalizer.”
That’s a powerful thought, given the indignity that confronts many Americans when they try to interface with the healthcare system at any level, including when they see their providers—whether the providers intend that or not. The hypothetical HACK app, simply by virtue of being an app, confers a sense of dignity that we might not get in the doctor’s office, or indeed anywhere else.
As a survey on dignified care put it, “Dignity is at the heart of personalization. Dignity means treating people who need care as individuals and enabling them to maintain the maximum possible level of independence, choice and control over their own lives.”
We live in an era where America’s healthcare system does not prioritize dignity. Is it possible to claw some of that back?
If you’re going to design a healthcare app to democratize healthcare access for people, that includes you.
In another Spicy Takes exchange, Stepro observes, “Isn’t it better when the consumer is educated and activated—after all, it’s our own body on the line? I’m glad folks are turning to Google or GPT for answers, even if they aren’t perfect, because it shows a healthier dynamic.” Behan responds that unvalidated or wrong information is hard to overcome, and Stepro sarcastically asks if misinformation in medicine has been a persistent issue.
Well, yeah, those problems face all of us, don’t they? We all consult with Dr. Google occasionally, because it’s free, and you can consult it at any hour and ask it any stupid question you want. The downside is that the answers aren’t reliable and can’t substitute for what an actual doctor might advise. And Dr. Google has no idea what your full medical history is (not that you want it to).
Some third-party apps like Ada Health improve dramatically on Dr. Google by using symptom checkers based on verified medical information. Chatbots based on large language models can certainly look up your ailments and dispense advice, although you should be wary if they encourage you to eat rocks. If you’re fortunate enough to have access to the Wolters Kluwer’s UptoDate clinical decision support service, you can find loads of evidence-based data refuting social misinformation. You can even get mobile access to it, and at $60 a month that’s not too shabby.
It’s still pretty far from “free,” however, and UptoDate doesn’t know whether you have a medical condition that could make any recommendations it offers highly dangerous. But if that feature is integrated into the HACK app, you lose the danger of uninformed recommendations, and get to keep the endlessly useful medical library.
On that subject, what else can we pack into this thing?
What an app wants, what an app needs
So far, the HACK app has two big features:
A library of trustworthy medical information that you can consult for any reason, at any time, that’s informed by your medical history included in the app.
Your entire medical history, including all lab results, hospital stays, specialist care, etc. regardless of which healthcare provider you saw for any of these treatments.
Let’s continue stealing important features from other smartphone apps to integrate them into the HACK app, bearing in mind that they must be for the individual using the HACK app—not features designed for providers to gather data from, or to influence the behavior of, the patients they treat.
What else?
Let’s say the app has an UptoDate level of education materials in a database that connects to your specific data and diagnosis using MedlinePlus Connect. Give the app a chatbot that can pull from this database to answer all of your questions, regardless of how sensitive or embarrassing, and deliver that information in simplified terms without jargon. Now you’ve got a semi-omniscient doctor in your pocket who can tell your uncle (or RKF Jr.) to stuff it when he goes on about vaccines causing autism.
Let’s say the app prioritizes having control over your own data and lets you update and make corrections to your EHR data using a souped-up version of OpenNotes. It also includes a data permissions management dashboard, with the ability to see an audit trail of who has accessed that information—even if there’s nothing you can do about it.
Let’s say the app can also be a buddy who just happens to have a weird fixation on making sure you follow your treatment plan. It incorporates behavior modeling tools from Health Catalyst’s UpFront app to take over remembering stuff when your brain is full (i.e., cognitive offloading). “Hey, you were supposed to schedule that colonoscopy three weeks ago—want me to go ahead and set up the appointment, ya big baby?” Okay, to be fair, Upfront would be nicer than that.
Let’s say the app can create a localized map of all healthcare providers and resources in your area that you can filter by available services. It builds this using tools like Unite Us’s resource directory or ZocDoc’s appointment booking platform, but no referrals are required—you self-refer. “Hi, I have a weird rash and need to see somebody within a week. What do you have available and how much is it going to cost?”
Let’s say the app also has a filter that flags conditions you have, and procedures you might need in the future that might become, you know, illegal in your area at some point. The app could tell you the next closest location where it’s still legal, and point to ride-sharing and other assistance to help you get there/afford it. It could even alert you to events like Texas Attorney General Ken Paxton suing HHS to slide past HIPAA protects to access data indicating you had an abortion.
For that matter, the app could shield you from (some of) the effects of federal cuts to health services with built-in compliance to existing regulatory measures that protect and preserve your data.
Let’s say the app has access to population health data showing the health risks you face most imminently and what you can do about them, incorporating those insights from Arcadia’s population health platform and Health Catalyst’s Ignite platform. The risks matter whether they’re nature or nurture, and you need to know ASAP what you can do about those affecting you.
Finally, let’s say the app, while placing all of this individualized information and these resources in a little device in your individual hand, also puts you in touch with communities of other human beings affected by the same conditions you are, by offering a feature like HealthUnlocked. You were never alone in this, and here’s the proof.
Nice little fantasy app you’ve got there. Who’s going to make it, though?
Ah, the mask has fallen. The jig is up. The cat’s out of the bag, and the deus is off the machina. What now?
Just kidding. This is a thought experiment for a reason—I don’t expect anyone to make the app. America is ripe for such an app, we need such an app, and we have the tools to create such an app—but that doesn’t mean we’re going to.
But let’s continue to be optimistic– perhaps I’m wrong on that second point. So, okay, what would developing the HACK app require?
A governing body to make sure the app is trustworthy
A sustainable funding model (Stop laughing– we just got started!)
Interoperability across all EHR vendors (I said stop laughing!)
Assume that we have satisfied all three requirements. This is, once again, a thought experiment.
Now, can we seriously address the matter of who makes the HACK app– and why?
What are our options?
The ONC
This one is obvious, because they already oversee FHIR and TEFCA, and interoperability is their dream. They also have regulatory power without a profit motive. But they don’t make software—they just regulate it. Somebody else would have to make it, and put the ONC in charge.
A private tech company (e.g. Microsoft, Google, Apple)
Microsoft attempted something similar with HealthVault, a site where users could store and share their health information, which fizzled and died in 2019.
Google Health was born in 2008, died, and then came back again, finally dying off for good in 2023.
But Apple Health is alive and kicking, using Fast Healthcare Interoperability Resources (FHIR) to let users import and view their health data on their iPhones and iPads after retrieving it. FHIR standards, importantly, were developed and adopted after Microsoft and Google made their respective shots.
When Microsoft and Google started leveraging FHIR, they were no longer in the “patient records for patients” business. Azure Health Data Services and Google Cloud Healthcare API are data platforms used by healthcare systems, payors, research institutions, and so on.
But in none of those cases was the focus on providing services based on patient records—just the records themselves. Apple Health can only function as a sort of meta-patient portal, requiring users to log into their actual patient portals to access their records, and their providers have to agree to letting Apple share the records in the first place.
If a private company like this developed the HACK app, you could argue that it democratizes access far more than the patient-portal-like products these companies previously developed, but, again—it would be their product, for better or worse, and arguably so would we.
A public-private partnership
This means:
Private tech company builds the infrastructure.
Nonprofit coalition manages the project.
ONC (or other federal agency) sets the standards and governs the data.
I guess that’s an option. But if this combination of entities could accomplish something like the HACK app today, why haven’t they done so already?
Who’s going to own it?
Taking on the project of creating the HACK app through that kind of partnership would be a tacit admission that the current system has failed, and that it’s going to take an app to save it—or at least, to survive in the face of that failure.
That’s the paradox of designing a “subversive” app promising to democratize healthcare through the backdoor, while only requiring access to all of the health records that healthcare systems are refusing to share right now, even after the ONC has hounded them to do so for over 20 years.
Each of the app’s features “stolen” from an existing technology really would have to be stolen, and it’s hard to imagine healthcare tech companies welcoming someone pirating their platforms.
On the other hand, it’s also hard to imagine a better example of the healthcare industry doing what it can to make a difference. “I helped someone understand their own medical records and make plans for future treatment today, when otherwise they wouldn’t have” is not nearly as sexy a claim as “I helped someone out of poverty today,” but it’s a lot more realistic– and on a higher scale, both of those claims could easily be true.
But because healthcare tech platforms sell patient engagement tools to providers rather than to people, there’s no motivation to develop a HACK app per se.
And even if the motivation was there, America has a population of—what—over 340 million at this point? How’s the HACK app going to reach all of us, even a large fraction of us?
How do we get this kind of reach?
Let’s assume that the HHS is developing the app—it would have to, to approach anywhere near that reach.
I’ve actually done a lot of research and writing lately about another app, developed by another U.S. federal governmental department, that reached as many as 64 million—while also stringently adhering to high security and data protection standards and relying on nationwide interoperability and data integration. It’s installed on my phone now, actually, though I’ll admit that I haven’t used it recently.
Maybe the HACK app could take some lessons from it?
Federal development and oversight—If HHS takes direct ownership of the app, just as this other agency did, that would mean developing the app in-house rather than outsourcing it to private industry.
Security and data protection—The HACK app would need to encrypt personal data, require strict user authorization as well as access control and permissions management, and comply with federal security standards, just as the other app did.
AI and automation for user navigation—Both apps rely on automated data processing, proactive notifications and engagement, AI-driven risk assessment, and smart eligibility and routing systems that guide users through decision trees based on their data.
Large-scale user support and infrastructure—Both apps must be scalable to handle millions of simultaneous users, both use mobile-first design, and both require redundancy and real-time threat monitoring for resilience against system failures and cyberattacks.
That’s a very general list of requirements, but if another government-developed app can succeed on this level, couldn’t the HACK app do the same? Assuming that the HHS has access to all information and other resources required to do it, that is.
Now, if your answer is “Yes,” how shocked will you be to learn that the other app is CBP One? You know, the app developed by Customs and Border Patrol to scan the faces of migrants and use that as a basis to determine if they can enter the country? The one that Trump shut down on his first day in office, forcing me to defend it after bashing it for months? Yes, that one.
I know, different government agency altogether. Different goals, altogether.
But that’s my point– regardless of how you think about immigration or healthcare, it says a lot that even after such an app was (successfully) developed to regulate immigration, it’s impossible to imagine the government developing a similar app to get healthcare access to Americans.
CBP One has something else in common with regular patient portal apps—it wasn’t developed for its intended end users, but rather the organizations providing the app. And as with patient portal apps, that didn’t stop government officials from boasting about how the app provides migrant empowerment—”There’s a lot of people who would love to migrate to the United States. In essence, they see CBP One as sort of a self-petitioning mechanism that we’ve never had before.”
*cough* So, anyway…
After all of this, have we democratized access to healthcare yet?
No, but we’ve shown that it’s possible to make a tool for getting there.
The U.S. in 2025 is a country:
where the best way to reach the greatest number of the population, regardless of demographics, is via a smartphone
with a disaster of a healthcare system that we have no choice but to navigate
where, within in that system, our healthcare needs are socially driven out of our hands
where huge advancements in healthcare technology have been made, and continue to be made, every day
whose government has already built a large-scale, high-security, interoperable app for mass data processing, supporting daily access by millions of people. Granted, that was for a very different purpose– but still, they did it
All of the problems standing in the way have been solved—just in different directions, for different people, with different purposes.
And now, the goddess Panacea would like a word.
She’s been quietly waiting in the wings, refusing to step anywhere near that cursed crane, even though she’s arguably the most qualified to do so.
She wants us to remember that America is now an older country than it ever has been, and older folks are sicker folks. They’re also notoriously bad with tech—but they’ve come far since the days when everybody was posting screenshots of their parents failing spectacularly at texting. And we’re at the point where the first generation to grow up using computers is eligible for AARP, anyway. So while the HACK app won’t replace their knees later on, it would be the next best thing to having a personal nurse (or tireless family member) with them 24/7.
She also points out that administrative efficiency is one of the categories included in the Commonwealth study where the U.S. tanked, with wasteful administrative spending estimated as high as $570 billion in 2019. And the HACK app could streamline patient access to records, real-time cost transparency, and insurance verification outside of the doctor’s office. Just sayin’.
Lastly, she wants us to know that the deux ex machina isn’t always what we think it is.
If your job is making boots, and you make boots for soldiers to wear to go to war, then boots are not your deus ex machina for winning the war. They’re just the tiny but significant contribution you can make, using the power and skills you have, to make winning the war more possible.
Likewise, if you’re in the business of making healthcare apps, your apps are not your deus ex machina for democratizing access to healthcare—they’re the tiny but significant contribution you can make, using the power and skills you have, to make democratized access to healthcare more possible.
She departs stage left with a warning: Stop hanging gods from cranes, she says. Just build some damn ladders, and let people climb.
The fear and despair I’m feeling right now are mostly due to three beliefs: that such killings a) might have been inevitable, b) will certainly only make things worse, and c) may well happen again.
Black Lives Matter is of course both a slogan and a movement, and the movement’s leaders have disavowed violence against police officers. But America is certainly fond of binary thinking of the “you’re with us or against us” variety. Onlookers have gathered in a circle around this conflict like a group of children yelling “Fight! Fight!” Especially those who have drawn a line of allegiance between BLM and The Police, and have donned their #AllLivesMatter, #BlueLivesMatter, and “I Can Breathe” t-shirts to signify which side they’ve chosen.
My friend Ed Brayton remarked that he was experiencing writer’s block in the wake of the murders of Alton Sterling and Philando Castille, followed by the killing of five police officers in Dallas. But he still managed to make the following observation that I think should be preserved:
This is not the least bit surprising to anyone who has paid attention to the problem over the years. And so we have the Black Lives Matter movement protesting against such injustice and brutality. And while you may dislike some of their tactics, they are right on the core issue. Our criminal justice system really is racist from top to bottom. Anyone who denies that cannot possibly have seen all the data that supports it, data that I have been presenting for more than a decade. And then we have two men who gunned down 11 police officers in Dallas on Thursday night, at the end of a long and peaceful protest against this injustice. What they did is horrifying and wrong in every possible way and it will do nothing but undermine efforts to address the problem. But unlike the unjust and racist treatment of black people in this country, that is an incident that is merely anecdotal, not systemic. But let’s also recognize that it was virtually inevitable. I have been saying this for years: When you oppress people, you radicalize them. If you do nothing to address legitimate grievances and fix problems, it is inevitable that some small portion of the victims of that oppression are going to choose violence as a response. That doesn’t justify it, but it does help explain it. If you cannot change as a result of non-violent protest, you make violent protest inevitable. And here’s the real problem: All this does is perpetuate the cycle of violence. Like the Hatfields and McCoys, every act of violence is then used to justify the next reprisal, which is then used to justify the next one, and the next one. At some point, the violence has to stop. But the only ones who can really stop it are those with power, which means law enforcement, courts and politicians. Violence on the part of those who protest against state-sanctioned killing is a response to the misuse of power, not an expression of power. It is up to those with power to fix this. No one else can.
What I fear is that Ed is right…but that those with power will not fix this. That they will just double down, using the killing of these officers as justification.
By all accounts, BLM and the police of Dallas actually had a decent relationship prior to the post-protest ambush, and hopefully will manage to repair that relationship in the wake of it. The same probably cannot be said of Baton Rouge. But that’s kind of the point– these things differ from state to state, city to city. Police departments have different approaches, including Richmond, California police chief Chris Magnus’s decision to stress de-escalation and the development of a positive relationship with citizens above all else.
All of which tells me that progress is being made on a local level. Quantifiable measures like the increase of police departments using body cameras are one way to recognize this, but of course body cams aren’t a panacea– no simple increase in accountability can be, though we still absolutely need increased accountability!
But what we also need, so very desperately, is a paradigm shift. Nationally, we have to recognize that being opposed to racism and brutality in a police force is absolutely not the same as being anti-cop (any more, as one meme noted, than being anti-child abuse is the same as being anti-parent).
We have to acknowledge that the more police officers are different and separated from the communities in which they operate, the more empathy for people in those communities is diminished. No police department is an occupying force. Every police department is composed of human beings entrusted with tremendous power and authority to enforce the law, who are still human beings. For better and for worse.
The “for betters” like the examples of Chris Magnus, like Wichita’s police chief Gordon Ramsay (yes, our police chief’s name is Gordon Ramsay and he’s organizing a cookout– what?) should be encouraged, rewarded, and perpetuated.
And when it comes to the “for worse,” to the biases and cover-ups and abuses…there are ways to counteract these. We absolutely must work to counteract these. Our local communities and our national community depend on it.
The BBC has a profile on Omar El-Hussein, the man who carried out Saturday’s killings in Copenhagen. He apparently was assisted by two other men, who have since been taken in police custody. They were charged with providing El-Hussein with weapons and helping him escape after the attacks.
We know El-Hussein was not an immigrant– he was a native Dane. He first attacked a gathering of people discussing free speech and blasphemy, and then a synagogue, in what looks like a clear attempt to emulate the Charlie Hebdo masscre in Paris in January (Charlie Hebdo offices in that case and then kosher market). Lars Vilks told the AP that he believed the Charlie Hebdo attacks “inspired” the shootings in Copenhagen.
According to the BBC, El-Hussein had in fact just been out of prison for two weeks before Saturday’s attacks. He sounds like a rabble-rouser and anti-Semite:
El-Hussein told psychologists he had a happy childhood and a good relationship with his parents and younger brother, according to a report obtained by Danish broadcaster TV2, but he failed to graduate from school or win a place at university. Classmates who spoke to the Ekstra Bladet newspaper (in Danish) remembered a loner with a hot temper who loved to discuss Islam and the Israel-Palestine conflict. He was not afraid to voice a hatred of Jews, said one. As a young man he was a criminal rather than a radical – reportedly arrested twice for possession of cannabis but let off with a warning. He took up kickboxing and began to smoke cannabis heavily. He was arrested once in a Copenhagen nightclub with a knife, and another time with brass knuckles – earning him a night in custody, according to Ekstra Bladet. But things took a much more serious turn in November 2013 when El-Hussein stabbed a 19-year-old man on a subway train. He evaded capture but was arrested by chance two months later in connection with a burglary, the Politiken newspaper reported (in Danish). He escaped an attempted murder charge, convicted instead of grievous bodily harm and sentenced to two years in prison.
I’m sure the response by many Americans to this would be that El-Hussein just didn’t sit in prison for long enough, but short prison sentences (compared to in America, that is) are normal in Denmark, and it has worked out pretty well for the country so far.
Rather, some people are arguing that the problem– at least, I hasten to say, concerning last weekend’s killings– may have been that he went to prison at all:
Prison guards in Denmark fear Hussein, 22, was the latest case of prison radicalization — in which criminals become devotees of militant Islam. Union leader Kim Østerbye said that Hussein had been housed in Copenhagen’s Vestre Fængsel alongside extremists including convicted terrorist Said Mansor, who had previously tried to radicalize other inmates. He said many young Muslim inmates at the facility were openly anti-Semitic and cheered in happiness at news of the massacre at the Charlie Hebdo magazine in Paris in January. He said they often chanted and called for the execution of cartoonists who depict the Prophet Muhammad. The prison service would not comment on the claims when contacted by NBC News. A reporter who covered Hussein’s assault trial told NBC News that the young man had seemed liked “just a hardened criminal” rather than an Islamist extremist before going to prison. “Omar, at the trial, didn’t seem religious at all. Almost the opposite,” Jesper Braarud Larsen said earlier this week. “He just seemed like a callous, hardened criminal … nothing more spectacular about him.”
Interesting phrasing there, when “religious” in this case means “interprets his Muslim faith to justify murdering Jews and blasphemers.” That isn’t the opposite of being a callous, hardened criminal at all, is it? That’s being a callous, hardened criminal whose choices of worthy targets of crime have shifted to focus on perceived enemies of religion.
Or maybe it wasn’t that much of a shift? The passion for Islam was already there. The anti-Semitism was already there. I can’t seem to find any further details about the identify of the 19 year old man El-Hussein was imprisoned for stabbing, but if he had also been a blasphemer or Jewish (or both) it wouldn’t exactly be incongruous with either El-Hussein’s previous character or his post-imprisonment terrorism.
It’s tempting to say that Larsen, the reporter, was valorizing religion– claiming that religious people are somehow by definition not criminals– but I think it’s more likely he meant that they are not petty criminals. That “spectacular” Islamist extremists are a fundamentally different sort of person than thuggish pot smokers who carry brass knuckles to clubs.
I’m afraid– really, this thought frightens me– that they’re not. That’s the banality of evil for you.
Yesterday a symposium to discuss blasphemy and the meaning of free speech was held at a cafe in Copenhagen called Krudttønden.
In attendance at this meeting was Lars Vilks, a 68 year old Swedish man upon whose head the Islamic State placed a $100,000 bounty for his 2007 depictions of Islamic prophet Muhammad as a “roundabout dog” (As a dog, basically. An Invasion of the Body Snatchers-reminiscent creaturestanding on four legs with a human head, bearded, wearing a keffiyeh).
A description of the event asked whether artists could “dare” to be blasphemous in the wake of attacks by Islamist gunmen in Paris last month against satirical magazine Charlie Hebdo. In an indication of the threat faced by the cartoonist, a note was included on the website saying there was always “strict security” whenever he spoke in public.
Inna Shevchenko of the Ukrainian feminist group FEMEN was reportedly speaking when the shots were fired. She said later:
I was talking about freedom of speech. I said that sometimes one has the illusion of being able to take advantage of this freedom, but it is an illusion and it is at this moment that we heard a burst of gunfire.
According to Jenny Wenhammer, who was in attendance [roughly translated]:
Gunfire when Lars Vilks Committee today held an international meeting in Copenhagen on “Art, blasphemy and freedom of expression”. During the Femen International’s leader Inna Shevchenko’s speech for two hours, then were fired 20-40 shot outside the doors and all started running. The French ambassador was also there to discuss Islam. Vilks was able to escape into a cold room, and Inna fled with others out through the back door.
The French ambassador, Francois Zimeray, tweeted during the attack that he was “still alive in the room.” One attendee, however, was not. The shooter reportedly fled the area in a black Volkswagon Polo while pursued by police, leaving behind one murdered civilian, Finn Norgaard, and three wounded police officers.
A few hours later and some miles south in Copenhagen there was another murder outside the Krystalgade Synagogue, of a 37-year-old man called Dan Uzan who was a member of the local Jewish community and was guarding the synagogue while a bat mitzvah was going on inside. Two additional police officers were shot and wounded in their arms and legs.
Copenhagen police reportedly killed el-Hussein last night after he opened fire on them in the Norrebro district. The officers had been staking out the address they had identified as his, and when he returned home he pulled a gun and fired on them. They returned fire and shot him dead.
Danish Prime Minister Helle Thorning-Schmidt did not hesitate to call el-Hussein’s acts terrorism, saying
We will defend our democracy. When the Jewish community is attacked, the whole of Denmark is attacked. The Jewish community does not stand alone. We don’t know the motive for the attacks but we know that there are forces that want to harm Denmark, that want to crush our freedom of expression, our belief in liberty. We are not facing a fight between Islam and the West, it is not a fight between Muslims and non-Muslims.
My friend and former colleague Anders Lisdorf, who lives and works in Copenhagen, had this to say:
Our company office is 100 meters away from where the “terrorist” apparently used to live and was shot. I have lived and worked in the area for 10 years. I like the neighbourhood a lot, so first of all I can tell you that most people are not terrorists, but in general very nice and decent people, so I am not afraid to go there tomorrow. I can also tell you that you cannot walk in peace with a jewish Kippa there, because you will be harassed by certain Muslim residents and violently so. The Mosques in the area have been known to preach a less than tolerant agenda. It is a poor neighbourhood with the typical problems of such a neighbourhood. The attacker was also involved in gangs and illegal gun possession. These problems are everywhere. In Norway it was a fundamentalist nationalist who was the terrorist (Breivik). The real issue is not the west versus Islam, I agree, but to protect tolerance and fight racism. We have to take issue with racists no matter whether they are Western Nationalists, Christian, Jewish or Muslim.
1. Obey the law, and you have nothing to fear. 2. Break the law, and you deserve to be tortured to death. 3. Rules #1 and #2 are applied equally to all Americans. 4. Police never break the law themselves. 5. When they do, they are never protected in ways civilians wouldn’t be.
Oh wait, I get it…this shirt is for police officers!
Breathe easy, cops– and hey, don’t break the law. But if you do, and murder one civilian after another in horribly gruesome ways, breathe easy…you won’t suffer the fate they did.
Justice system ignored facts I don’t know whether to feel saddened or enraged from reading about the man choked to death on a New York City street. The sources indicate this type of restraint by law enforcement officers was banned 20 years ago, yet a Staten Island grand jury saw no problem with the outcome of the officer’s action (Dec. 4 Eagle). Quite a few years ago, I was hired to be the summer school librarian at an alternative high school in Wichita. An African-American student came in frequently to finish up his homework, so we began to share stories. One day he revealed that the glasses he wore were just plain glass. He said he wore them so he would look less threatening. On more than one occasion when he entered an elevator, a woman would get off rather than share the space with him. He hoped the glasses would render him less aggressive-looking. I have never forgotten his story. Evidently, after all these years, we haven’t made much progress in seeing past a person’s color. I see myself as a problem solver, but I cannot come up with a solution to the problem of a justice system that can ignore facts with such a degree of capriciousness. SUZANNE KOCH WICHITA
Suzanne Koch is my mom. Did I mention that my mom is amazing?
Or, why good storytelling requires good representation:
When the story doesn’t contain the “why,” the audience looks to the author.
Let me back up.
Writers are often advised to “write what you know.” That’s good advice, because you can’t write believably about what you don’t know. However, authors who took this advice to a logical extreme and wrote only about people just like themselves would suffer for it. They wouldn’t tell very interesting stories– or at least, they would have only one interesting story to tell, and it would effectively be a memoir.
Rather, fiction writers write what they know by research. If they want to write a story about a marine biologist, they would research marine biology. They would research what working as a scientist in that field is like, what kind of person goes into that field, what kind of education and training it requires, and so on.
Because even though it’s fiction, believability is key. Fiction writers create worlds that are not identical to this one for the entertainment of the reader, but those worlds contain things that exist in our own world– like people. If the people in the story don’t act like people do in the world world, and no reason is given for this, the audience is confused. The story falls flat. It’s bad storytelling.
So this is a kind of constraint on the author. When writing fiction it’s literally true that an author can write any story he or she wants– nobody is going to come in and hold a gun to his/her head and demand that he/she not write the story. However though the author is entitled to write whatever story he/she chooses, he/she is not entitled to the audience’s reaction. The audience is not required to think highly of the story. The audience is not required to think highly of the author.
As an example, imagine an author who writes a book whose story involves the sole white occupant of a town being lynched by the rest of the town’s population, which is black. If a believable explanation for this plot line can’t be found in the story, the audience is going to guess that either the story is satire, or the author has some serious issues with black people. Their likelihood to understand the story as satire is a blend of their own knowledge and the author’s adeptness at storytelling. Bad satire happens when the audience can’t be expected to have the knowledge that will tip them off to its satirical nature, or when the author doesn’t wink hard enough in the writing of the story to make it clear. Or both, of course. When the audience doesn’t detect satire (it doesn’t provide the “why,”) then they quite reasonably look to the author’s own beliefs for the explanation.
Good storytelling involves researching the elements in your story if you don’t know very much about them. Bad storytelling involves misrepresenting those elements or leaving them out altogether in a way that isn’t believable. An author who wants to tell a story about a world congress, in which multiple leaders from every country gather together to exchange ideas, isn’t practicing very good storytelling if his/her story depicts this congress as containing only white men, unless a reason is given for this. Was there some mass extinction of women and people of color? Did the white men totally take over the world, including the government of every country on the planet, and if so….how did that happen? The extraordinary event requires an extraordinary explanation. In fact in this case, it would be such an extraordinary explanation than it might as well be the story. If it isn’t, but is treated as a totally unremarkable circumstance by the characters in the story, the audience would rightly look to the author with a “WTF?” expression on its collective face.
These examples are extreme, but that’s on purpose– to illustrate how the content of a story can lead the audience to negative conclusions about the beliefs and prejudices of its authors. The less cut and dry it is, obviously the less justified the audience would be in reaching these conclusions. But the audience is not wrong to see an unbelievable depiction of people in a story and assume that the explanation lies in the author’s motives, and they’re going to do it regardless.
The first people to notice when certain groups of people are misrepresented in or left out of a story for no discernable reason are, quite naturally, people in those groups. But they’re not the only people who do notice or should notice. It might take a white guy a little longer to look at the “world congress” and think “Hey, wait a minute….why is it only people like me?” But he wouldn’t be very bright if he never got there. Not very bright, or else like the author in either prejudice or ignorance (or both).
People want to hear stories told about people like them– yes, of course. However, people also want to hear good, believable stories. If a story makes you stop and wonder why the author portrayed characters in a way that rings false, or leaves them out altogether when it seems like they should be there, that’s bad storytelling unless making you wonder these things is the author’s point– and even then, if you can’t tell whether it is or not, that’s a problem.
That’s why diversity matters in storytelling– not just because people want to hear/see it, and they do, but because it makes the story better. Because the story contains the “why.”
First, I didn’t talk at all yesterday about the statement of motivations in The Marriage Vow that preceded its fourteen provisions, which included two claims that have since been removed:
Slavery had a disastrous impact on African-American families, yet sadly a child born into slavery in 1860 was more likely to be raised by his mother and father in a two-parent household than was an African-American baby born after the election of the USA’s first African-American President.
LBJ’s 1965 War on Poverty was triggered in part by the famous “Moynihan Report” finding that the black out-of-wedlock birthrate had hit 26%; today, the white rate exceeds that, the overall rate is 41%, and over 70% of African-American babies are born to single parent.
Um, Hell-to-the-yeah slavery had a disastrous impact on African-American families. White slave owners broke apart families to sell, raped black women, and often confiscated the babies from these forced unions. Somehow, conservatives like Bob Vander Plaats forget to mention that. They are too busy buying into the fake history of the forefathers from WallBuilders. The statement that a child born into slavery in 1860 was more likely to be raised by his mother and father in a two-parent household is a boldfaced, ignorant lie, designed to tug at conservative white heartstrings and sucker in some African-American Christian conservatives. To wit, let me quote Frederick Douglass from his autobiography: “The practice of separating mothers from their children and hiring them out at long distances too great to admit of the meeting, save at long intervals, was a market feature of the cruelty and barbarity of the slave system… It had no interest in recognizing or preserving any of the ties that bind families together or to their homes” I am really getting sick and tired of the conservative meme about saving marriage, and placing the shaky foundation of their argument on African-American single parent birth and wedlock rates. Conservatives idolize the founding fathers, yet they conveniently forget the legacy of slavery and its atrocities many of the founders acquiesced to. While conservatives tick off statistics about African-American babies born out of wedlock, Teen Mom is the MTV show where teenage white girls can get their cash on by being pregnant and beating up their boyfriends on TV. Bristol Palin is proof that being a pregnant, unwed white girl is enough for a memoir at 20 called Not Afraid of Life. Put this together with all the reproductive rights rollbacks on abortion and the like, and the schizophrenic hysteria of the right doesn’t hold up. When it comes to vows, pledges, and the like, the last thing I want to hear it from is a white male conservative authoring some sappy pledge for candidates to sign. After reading the report on John Ensign and Mark Sandford hitting the Appalachian Trail, and the RNC using funds at a sex-themed voyeur nightclub, moralizing, asinine pledges aren’t going to stop anyone, including the candidates, from having sex and watching lots of porn. Add in the ahistoricism of the right, and it’s laughable that any pledge from this hypocritical bunch could hold water.
I don’t think I have anything to add to that.
Also, today Salon published an interview with The Family Leader founder Bob Vander Plaats, who authored The Marriage Vow, including apparently the worst photo of him they could find. I’m really not a fan of that, even when the person in question is someone I despise. Some background on TFL generally Vander Plaats specifically:
The Family Leader was formed after the 2010 elections as a coalition of Iowa social conservative advocacy groups, with Bob Vander Plaats as its executive director and public face. Vander Plaats had become the best known conservative culture warrior in Iowa that year after receiving a respectable 41 percent of the vote in the GOP gubernatorial primary; his campaign focused on reversing a 2009 decision by the state supreme court allowing same-sex marriage. After losing in the primary, the fiercely anti-gay Vander Plaats led the successful campaign to oust three supreme court justices who had voted for the same-sex marriage decision. Now at the helm of the Family Leader, he has brought in presidential hopefuls for a speech series and is openly cultivating an image as Iowa kingmaker.
When asked whether TFL’s support hinges on the matter of whether or not a candidate would sign the Vow, Vander Plaats replied:
What we’ve said is that a primary candidate for the office of president will not get our support if they can’t sign this pledge. If they can’t sign the pledge, we’re going to ask them questions like, “Where’s the issue you have with the pledge?” Because we want to have a discussion and a debate. And if for any reason they point out something we’re just wrong on, then we’d admit it and say “OK, we’re wrong on that.” But we don’t see that.
Are you surprised? I’m not surprised.
Regarding the plank concerning Sharia Islam:
There’s one section in the pledge that says the candidate has to reject — the phrase used is “Sharia Islam” — can you describe what you mean by that phrase and what you want the candidates to reject in that? Well, Sharia Islam — and I’m not an expert on Sharia Islam — but I think just in the brief knowledge [I have] of Sharia Islam, one you can have multiple wives, and two is you can have temporary wives, and three is I think it disrespects women as a whole. And so we see Sharia Islam as being an issue.
Only a “brief knowledge,” yet apparently it is such a threat that it must be specifically mentioned in a statement on protecting marriage that presidential candidates are being asked to sign. Got it. Are we supposed to assume that the candidates know more about Sharia than Vander Plaats does?
Regarding pornography:
Another part of the vow that’s gotten attention was the clause about promising to protect women and children from a long list of evils. Some of those things were obviously crimes — human trafficking was one — but there was also pornography. What would you say to people who don’t see pornography as a threat to women? And secondly, do you think only women need to be protected from pornography or should men be, too? Well I think if you read in that, there’s also the word “coercion” — “coerced.” I don’t have the vow in front of me right now, but I think if you read that it’s going to talk about coercion as it relates to abortion, prostitution, pornography. What we’re trying to do is have a high standard for women and for children, as well as for marriages and for family. Some people were saying that the pledge was somehow calling for a ban on pornography, is that what it was intended to do? No, not at all. I think if the Family Leader could have its way, we’d probably say we’d like to have a ban on pornography. But that’s not the vow. The vow was [about] forcing women into pornography.
Really? Let me remind you, Mr. Vander Plaats, of what the vow you authored actually says on that:
Humane protection of women . . .from all forms of pornography. . . and other types of coercion or stolen innocence.
Sure sounds to me like you’re defining pornography as a form of coercion, or at least “stolen innocence” (whatever that means), from which women need to be “protected.” Suddenly consent matters! Just not enough to make it clear in the document presidential candidates are being expected to sign, apparently.