The intersection of healthcare and immigration policy is found in the halls of hospitals and clinics across America, where increasing numbers of International Medical Graduates (IMGs) are filling in for doctors who won’t return, and state governments are doing their best to usher IMGs into practice where they’re sorely needed.
Help (Badly) Wanted: Foreign Doctors Apply Within
In 2023, Tennessee became the first U.S. state to drop residency requirements for some IMGs,1 giving them a new pathway to permanent licensure. Following Tennessee’s (somewhat surprising) lead, at least 15 states have introduced legislation to create streamlined pathways to medical practice for IMGs, with both Republican and Democrats contributing.2
During the 2025 state legislative sessions, over 20 bills have been introduced that would expand opportunities for IMGs to support America’s healthcare workforce needs. These range from allowing qualified DACA recipients to apply for licensure in New York to removing redundant training requirements in Montana.3
Some state legislation is more focused in scope. For example, in Illinois, IMGs must not only be legally able to work in the U.S., but are also mandated to work in medically underserved areas.
Perhaps most shockingly, in 2024 Governor Ron DeSantis of Florida signed the “Live Healthy” initiative to allow IMGs to bypass residency requirements if they have equivalent training experience. But then, the largest population of IMGs is in geriatric medicine, where they make up more than half of the physician population. And, well, it’s Florida.
Already at their shift
For that matter, according to the American Medical Association, a full 25% of licensed U.S. physicians are IMGs,4 with the largest number coming from India, followed by the Caribbean, Pakistan, the Philippines, and Mexico.
This is where the cognitive dissonance comes in– or at least, it should.
The new administration’s condemnation of everything related to equity and diversity, coupled with its rabid pursuit of an America free from immigrants, is simply incompatible with this reality. The reality is that massive numbers of the country’s doctors come from foreign countries, and are supported by legislation and advocacy work focusing on combatting racial and ethnic disparities.56
The AMA’s International Medical Graduate (IMG) Toolkit, in its section on “Academic opportunities and scope of practice,” acknowledges the fact that IMGs will face discrimination, but encourages them to press forward:
IMG physicians face several barriers in their goals and aspirations towards a career in academic medicine. . . Systematic exclusion is also a reason leading to discrepancies in leadership positions and promotions among IMG physicians. Despite challenges, IMG physicians are encouraged to choose an academic career as diversity is a strong determinant of innovation in medicine.”7
Those words “strong determinant” stick out to me, having written so much about social determinants of health.8910
A strong determinant doesn’t make a result inevitable, but rather highly likely. “You have something to contribute,” this guidance says, “So don’t give up in the face of discrimination. Keep trying, because we need you.”
I wonder if America is aware of how much we need IMGs, and how opponents of “DEI” and immigration reconcile their views with this reality.
Wait, actually I don’t. The reality itself is what matters– it’s where IMG physicians can, and do, make an enormous difference.
The language used to justify policy is…fraught. Every new program is a triumph, as is every cut to an existing one. Every new rule is a sea change, and every executive order a roadmap to utopia. These flowery-but-decisive statements come from all politicians, pointing in all directions, and they always have.
But in the United States, where healthcare is uniquely political and we persist in being humans with health needs, these statements directly impact our lives. We must pay attention. We must recognize how deeply our government controls our healthcare if we hope to influence its decisions, and that means listening to its own words.
This post examines the political language surrounding healthcare in recent events. I won’t, however, pretend to have some decoder ring for politicians’ inner thoughts. I don’t need one—their intentions are right there in plain language. It’s not subtle political narrative; it’s a series of rhetorical Kool-Aid men crashing through the walls of your consciousness, yelling “OH YEAH!” every time. Every. Single. Time.
“Lowering costs”
For example, the Trump administration recently issued an executive order “to empower patients with clear, accurate, and actionable healthcare pricing information.”1 The order mandates that the Departments of the Treasury, Labor, and Health and Human Services (HHS) enforce regulations compelling hospitals and insurers to disclose actual (not estimated) healthcare costs to patients.
The goal is “lowering costs for American families.” “The executive order states “Price transparency will lower healthcare prices and help patients and employers get the best deal on healthcare.”2
Enforcement of these regulations falls to the Centers for Medicaid and Medicare Services (CMS) within HHS, using three main avenues for monitoring compliance. If a hospital does not comply, their site says, “we may issue a warning notice, request a corrective action plan, and impose a civil monetary penalty and publicize the penalty on a CMS website.”3
To be clear, I think healthcare pricing transparency is a great idea.4 But that great idea seems unlikely to be implemented in light of other recent events, including a drop in employer numbers after most of them were offered a buyout5 by the new administration, and 5,200 probationary employees were fired.6
Perhaps that administration has determined that the CMS will have extra spare time and funding to check compliance as it abandons a foundational and essential goal on the basis of sheer ideology– but we’ll get to that below.
Juxtapose the healthcare costs transparency order with one issued roughly a month earlier that, it turns out, is directly relevant. On January 20, Donald Trump mandated that the federal government should:7
Terminate, to the maximum extent allowed by law . . . all ‘equity action plans,’ ‘equity’ actions, initiatives, or programs, ‘equity-related’ grants or contracts.”
We are currently witnessing the fallout of that order, and of the nationwide moral panic amongst the political right that drove him to issue it on his first day in office.
“Eq*ity”
But what does this allegedly dirty word even mean, in the context of healthcare?
The goal of achieving health equity was articulated by the previous administrator of the CMS, Chiquita Brooks LaSure, in the CMS FY2025 performance plan:8
As the Nation’s largest administrator of health benefit programs, CMS is uniquely positioned to accelerate initiatives that advance the Secretary’s commitment to enhance mental health services, transform pandemic preparedness capabilities, and advance health care quality. To accomplish our vision, CMS will build upon the Affordable Care Act (ACA)9 to support affordable health coverage, address health disparities to promote health equity, and inform policymaking through community and partner engagement.
And (for now, at least) the CMS.gov website defines health equity in this way:
The attainment of the highest level of health for all people, where everyone has a fair and just opportunity to attain their optimal health regardless of race, ethnicity, sexual orientation, gender identity, socioeconomic status, geography, preferred language, or other factor that affect access to care and health outcomes.10
How long has the concept of health equity been around? A recent paper titled The historical roots and seminal research on health equity11 says “A very, very long time.”
Research on health equity experienced three important historical stages: origins (1800–1965), formative (1966–1991) and development and expansion (1991–2018). The ideology of health equity was endorsed by the international society through the World Health Organization (1946) declaration based on the foundational works of Chadwick (1842), Engels (1945), Durkheim (1897) and Du Bois (1899).
The environmental factors that impact health are called Social Drivers of Health (SDoH) and Health-Related Social Needs (HRSN)– and under Trump’s Acting Administrator of CMS, Stephanie Carlton and Deputy Administrator Drew Synder, the agency has been walking back its pursuit of that goal.
An “ideological crusade”
As of March 4, The Centers for Medicare & Medicaid Services (CMS) has pulled information on health equity for the Medicaid and Children’s Health Insurance Program (CHIP) through Section 1115 waivers,12 a move that former chief medical officer for the Medicaid program at CMS Andrey Ostrovsky, M.S. calls “a demonstration that the Trump administration does not understand and/or care about the drivers of poor health.” “Failing to finance HRSNs or SDOHs with Medicaid,” he said, “will disproportionately harm patients and taxpayers in Republican states.”13
Senator Ron Wyden of Oregon was more blunt, accusing newly-minted Secretary of HHS Robert Kennedy of an “ideological crusade against Medicaid.”14
Services that CMS has provided coverage for, based on HRSN data, include home accessibility modifications like handrails and wheelchair accessibility ramps, transportation vouchers, rent or utility assistance, and care coordination– helping individuals manage their care plans.
What’s the justification for the change? A memo15 by Snyder states:
To support implementation of coverage of certain services and supports to address “health-related social needs” (HRSN) in State Medicaid programs and Children’s Health Insurance Programs (CHIP), the Center for Medicaid and CHIP Services (CMCS) issued two Center Informational Bulletins (CIBs). The first. . . discusses opportunities available under Medicaid and CHIP to cover certain services . . .that purport to address HRSN. . . To evaluate policy options consistent with Medicaid and CHIP program requirements and objectives, CMS is rescinding the November 2023 and December 2024 CIBs.
“Purport”
In other words…no justification. Not even an attempt– just “We no longer care about this. Because, that’s why.”
But that little word “purport” in there fascinates me. Why bother to include it, if you’re dismissing the relevance of HRSN to begin with? Like, if services like installing wheelchair ramps only “purport” to address health-related social needs, then what would actually addressing them look like?
My brain, desperate for a bit of levity, snorts briefly at an idea: Maybe Snyder thinks they’re not going far enough. Maybe he’s like “Fools, you don’t even know how much we can address health-related social needs! Watch me cook!” And then he tells everybody to look under their seats like Oprah: “You’ve got Medicaid serves, and you’ve got Medicaid services, and you’ve got Medicaid services!”
Sadly unlikely, but I sure wouldn’t mind living in that universe.
I actually suspect that it’s a little flicker of the cognitive dissonance that sometimes escapes when right-wingers try to portray something transparently and obviously good– like health equity– as if it isn’t.
Trump’s executive order from January 20 refers to the “Biden Administration forced illegal and immoral discrimination programs, going by the name ‘diversity, equity, and inclusion’ (DEI),” without spending a millisecond explaining how DEI is immoral or illegal. Why? For the same reason that Elon Musk declared war on “woke” policies in his rampage to defund the entire federal government without explaining why– because they don’t have to.16
“Make America Healthy Again”
Let’s go back to CHIP for a moment. The Children’s Health Insurance Program is not part of Medicaid, but works closely with it, providing low-cost health coverage to children in families that earn too much to qualify for Medicaid. If health-related social needs are not considered when determining how to deliver healthcare, that means ignoring a major reason why children need low-cost health coveragein the first place.
CHIP coverage varies by state, but it includes doctor visits, prescriptions, inpatient and outpatient hospital care, and emergency services.17
Why do kids need all of those? Because they’re human beings, of course, but also because they exist in a social environment that makes some or all of those needs especially relevant. Some examples:
Housing Instability: Children in unstable housing have higher rates of asthma due to exposure to mold, pests, and poor ventilation.
Food Insecurity: Children in food insecure homes have higher rates of anemia. Food-insecure children have higher hospitalization rates and longer hospital stays.
Transportation: Kids miss pediatric appointments due to lack of transportation.
Health literacy gaps make parents more vulnerable to vaccine misinformation
An assessment of the latest CDC National Immunization Survey data found that more than one-third of U.S. children between the ages of 19 and 35 months were not following the recommended early childhood immunization schedule. Furthermore, a 2019 national survey found that approximately 1 in 4 parents reported serious concerns towards vaccinating their children. Vaccine hesitancy is now associated with a decrease in vaccine coverage and an increase in vaccine-preventable disease outbreaks and epidemics in the United States.
Oh, and there’s that measles outbreak in West Texas:19
Texas health department data shows the vast majority of cases are among people younger than 18: 39 infections are in kids younger than 4 and 62 are in kids 5-17 years old. Eighteen adults have measles and five cases are “pending” an age determination. . . Most kids will recover from the measles if they get it, but infection can lead to dangerous complications like pneumonia, blindness, brain swelling and death.
That’s from the AP, who took the time to directly refute our new Secretary of Health and Humane Services:
The MMR vaccine is safe and highly effective in preventing measles infection and severe cases of the disease. . .
Before the vaccine was introduced in 1963, the U.S. saw some 3 million to 4 million cases per year. Now, it’s usually fewer than 200 in a normal year.
There is no link between the vaccine and autism, despite a now-discredited study and health disinformation.
“But I do have reservations with your past on vaccines”
And yet Robert Kennedy, who made a promise to Sen. Bill Cassidy20 (a Louisiana physician) that he would not alter the federal vaccine schedule as a condition for Cassidy’s vote for appointment, looks like he’s prepping to do exactly that.21
Speaking for the first time to thousands of U.S. Health and Human Services agency employees, he vowed to investigate the childhood vaccine schedule that prevents measles, polio and other dangerous diseases.
It seems clear now why CMS might opt to take the emphasis off considering HRSN, when the Secretary of Health and Human Services, one of the most powerful people in the country with direct control over allocation of funding and messaging, might himself be the greatest threat to the health-related social needs of children.
“Nothing is going to be off limits”
That’s what he said regarding the scope of his so-called investigation, including inquiries into the effects of pesticides, food additives, microplastics, antidepressants, and “electromagnetic waves emitted by cellphones and microwaves.”
But in reality, he’s referring to children’s’ lives. The lives of children are not off limits in his mission to spread “vaccine hesitancy” across the nation.
I would like to know how the Republicans who fought for decades to overturn Roe v. Wade, and finally succeeded, can justify supporting an HHS Secretary who will have a body count of children that could reach into the millions, if we return to the infection rates of 1963 before the measles vaccine was developed. Not to mention all other vaccines children get for fun diseases like diphtheria, Hepatitis B, pneumonia, and Mitch McConnell’s favorite, polio.22
But hey, at least the fortunate children of parents who want them to be vaccinated, but who can’t afford it, can still get vaccinated through the Vaccines for Children program.23
Yes, the legislation that Republicans tried 70 times to “repeal and replace,” and that Trump still claims he has a “concept of an idea” for what should replace it. ↩︎
And given that these slogans-turned-smears all originated in helping people of colors other than white, it doesn’t take a space rocket surgeon to discern the true reasons for failing to elaborate. ↩︎
One of my first-year classes in college was History of Theater, in which I learned how the Greeks built amphitheaters into hillsides, carving out a semicircle of seating for the audience around the stage to maximize. The scenery for a play completes the circle, just as it does for any show in an amphitheater today. It’s the structure providing the necessary atmosphere for the experience.
Imagine sitting in such a theater, watching Euripides’ Helen, and seeing the demigods Castor and Polydeuces (Helen’s pissed off brothers) descend into the scene by a wooden crane—a mechane — whereupon they put an end to all of this murderous nonsense, and everybody lives happily ever after. It’s a literal top-down solution.
That’s where the expression deus ex machina, or “god from the machine,” comes from. And it became used, and mocked, throughout the world of fiction as a plot device providing a too-convenient, cheap ending to a story.
But my mind just keeps going back to that silly crane. It used to dangle a man dressed as a god before the audience, but these days he’d more likely be a techbro holding a smartphone, probably talking about the wonders of AI.
That’s on my mind today because in this post, I’m about to dangle a hypothetical mobile app in front of my audience– you. I illustrate our country’s mess of a healthcare system, and perhaps even reckon with it. This play isn’t ending any time soon, and we need to find a role in it (else one is chosen for us).
Healthcare data and analytics company Arcadia recently launched its own talk show, Spicy Takes, to discuss “hot perspectives in healthcare” while sampling—you guessed it—spicy food. The first episode placed President and CEO Michael Meucci in conversation with Chief Product and Technology Officer Nick Stepro and Chief Medical Officer Dr. Kate Behan.
I watched it while reading about their SDoH (social determinants of health) package, which promises to justify the time and expense required of providers to consistently record SDoH data by creating registries mapping that data with diagnostic codes, for use in proactively identifying patients at risk and connecting them to resources. While looking over the tear sheet, I heard Meucci say this:
I think that this is such a great platform for digital health as we start to think about how do you democratize access. Because if a patient is concerned that they’re not going to get the right treatment because of the color of their skin or the community they live in, the smartphone is a great equalizer. We talk about what’s changed for the last 10 years—that, to me is the biggest thing, the fact that you can pull out your phone and get connected with a doctor in 15 minutes.
“To your point, Stepro replied, “all of the technology and all of the access to healthcare in the world doesn’t change the fact that the single worst diagnosis you can have as a patient is being poor. You can’t address that with a healthcare institution. We can measure that poor people have lower outcomes but ultimately, we need to find and attack the problem of homelessness and poverty because you can’t just solve that in a clinic or with a smartphone.
I stopped reading and played that section of the show again. Meucci didn’t say that the healthcare industry can solve poverty with smartphones; he said we could democratize healthcare access. If that’s a spicy take then you can call me Spice Girl, because that’s my healthcare platform now. But I suppose coming from someone like him, that’s practically revolutionary.
And he’s right. As a country, America is primed for solutions like that: over 91% of Americans have smartphones. Even households without broadband hang on to their smartphones, because of course they would—it’s a tiny computer that can do more than any of us ever seem to realize, or ever will.
Democracy—another word with ancient Greek origins– literally means “power in the hands of the people.” What would it even look like to do that with a smartphone?
Let’s do a thought experiment to find out.
Time to design a smartphone app.
Imagine that in the beginning of The Legend of Navigating the American Healthcare System, our player character is given their first smartphone.
On that phone there’s an app installed (that I’ve just invented) called HACK: Health Agency, Care, and Knowledge.
Health – A full, patient-owned medical history
Agency – Control over your care, your records, your choices
Care – The power to find, compare, and advocate for treatment
Knowledge – Because to be informed is to be empowered
Does your vision of this app include it conferring access to all of an individual’s health records, stored securely but also accessible in their entirety at any time? If so, you’ve envisioned something better than what existing patient portal apps currently provide.
So yes, let’s absolutely start there, if we’re designing an app that democratizes healthcare in America.
And remember that democracy means that the power is in the hands of the people—not the “patients.”
Problem: we’re not in the driver’s seat.
Social Drivers of Health (SDoH) is the category of data on an EHR encompassing the non-medical factors affecting an individual’s health. In other words, your life, from the hospital where you were born (if you were born in a hospital) to the destination of your organs when you die.
They’ve been called the social determinants of health, but the word “determinant” suggests finality, immutability—that there’s nothing you (or anyone) can do about it. A driver, on the other hand, suggests that while the deck may be stacked against you, things could always change.
How easily could you could do that? *shrug* It depends, but we can safely say that “resident of the United States” is not an easy “driver” to change. We’re driving that road whether we want to or not.
And I hate to break it to you, but we live in a hostile health environment.
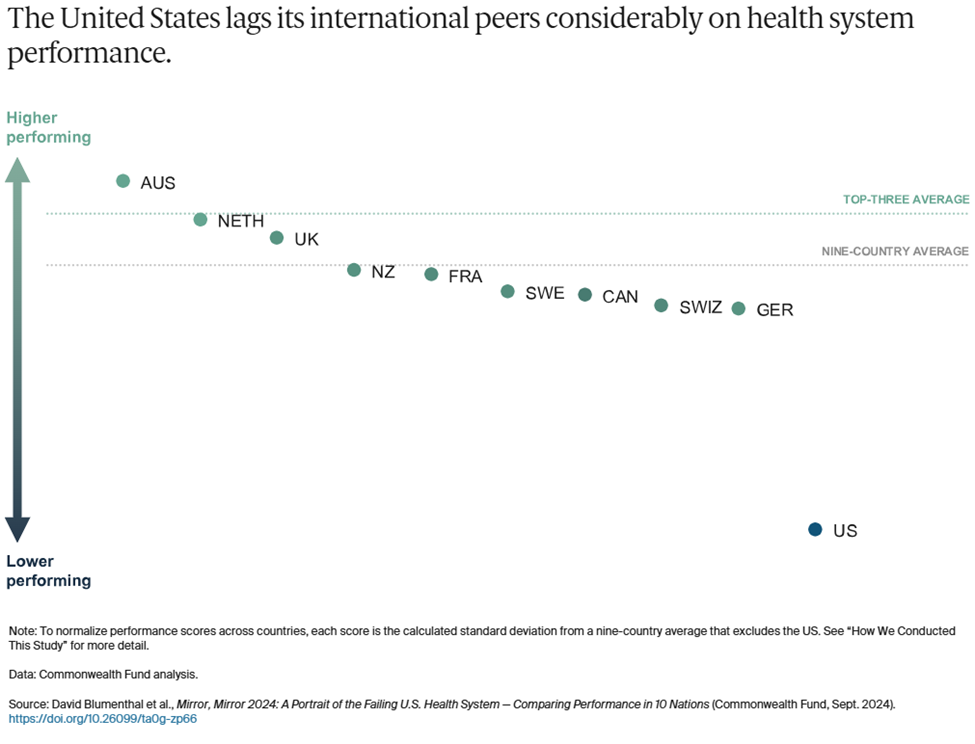
A 2024 study titled Mirror, Mirror 2024: A Portrait of the Failing U.S. Health System was conducted by The Commonwealth Fund to understand why America is doing so poorly by comparison—that is, going beyond the factor that rhymes with “schmooniversal schmealthcare.” The categories they used are:
Access to Care
Administrative Efficiency
Equity
Care Process
Health Outcomes
In all but one of those categories, America comes in dead last or next to last.
To summarize the report, it found that Americans spend more on healthcare as a percentage of GDP to receive lower healthcare system performance than other countries. It faces the most barriers to accessing and affording healthcare. Its physicians and patients are most likely to face hurdles related to insurance rules, billing disputes, and reporting requirements. Equity in healthcare access and experience is low. And we live the shortest lives and have the most avoidable deaths. All by a longshot. USA! USA!
The one exception in these categories is Care Process, where we came in second. Their comments:
Care process looks at whether the care that is delivered includes features and attributes that most experts around the world consider to be essential to high-quality care. The elements of this domain are prevention, safety, coordination, patient engagement, and sensitivity to patient preferences.
I interpret this result as an indication that some version of enabling people to take charge of their own healthcare is key to accessing that care in spite of all other factors. It could even, possibly, raise America in those other categories where we’re currently ranking dead last!
Okay, probably not, but it could definitely help us face the hostile health environment in which we currently exist:
Misinformation is everywhere.
We live in an era where vaccine misinformation spreads faster than the viruses they prevent, leading to the resurgence of eradicated diseases, overwhelmed hospitals, and preventable deaths fueled by fear rather than science.
We live in an era where people google their symptoms and often reach the worst, scariest conclusions that inadvertently contribute to their paranoia, where “doing their research” on healthcare can lead to being convinced of conspiracy theories and pseudoscience.
We live in an era where the president of the United States once advocated for injecting disinfectant as a means of staving off Covid, and in his next term has appointed a raw-milk-drinking anti-vaxxer as Secretary of the Department of Health and Human Services.
We live in an era where social media influencers with no medical expertise gain massive followings by promoting unproven “natural cures,” convincing people to reject evidence-based treatments in favor of detox teas, essential oils, and dangerous fad diets
We can’t afford anything.
We live in an era where Cost-Related Nonadherence (CRN) is the primary reason for medical nonadherence (failure of patients to take their medication as prescribed due to cost) in some cases forced to choose between “treating and eating.”
We live in an era where the term “dual ineligibility” refers to the status of undocumented immigrants in the U.S. who qualify for both Medicaid and Medicare, but are unable to access either one.
We live in an era where medical debt is the leading cause of personal bankruptcy, where a single hospital visit can trap families in a cycle of financial ruin, and where crowdfunding platforms have become a substitute for a functioning healthcare system.
We live in an era where rural hospitals are closing at alarming rates, leaving entire communities without nearby emergency care, prenatal services, or even a local doctor, forcing low-income patients to travel hours for basic medical attention they still might not be able to afford.
Neighbors hate and fear their neighbors.
We live in an era where in transgender healthcare, patients frequently encounter providers who lack adequate knowledge of gender-affirming care or hold prejudiced views that hinder appropriate treatment.
We live in an era where in reproductive healthcare, political and ideological barriers, including misinformation and ignorance, stand in the way of basic, safe medical care.
We live in an area where Black patients are more likely to have their pain underestimated and undertreated, leading to worse health outcomes.
We live in an era where in disability healthcare, patients struggle to have their pain, symptoms, and autonomy taken seriously, with providers sometimes dismissing concerns as psychological or unavoidable aspects of their condition rather than treatable medical issues.
We live in an era where in chronic illness care, patients—especially women—are more likely to be dismissed as exaggerating their symptoms, leading to years-long delays in diagnosis for conditions such as endometriosis, fibromyalgia, and autoimmune diseases.
We live in an era where in elder care, aging patients often have their autonomy disregarded, with medical decisions made on their behalf without full consent, reinforcing the notion that age diminishes a person’s right to control their own body and treatment.
We live in an era where fat patients are often told to lose weight as the solution to every health issue, leading to delayed diagnoses and overlooked conditions that have nothing to do with body size.
We live in an era where for immigrants, language barriers, lack of documentation, and fear of discrimination or legal consequences discourage people from seeking medical care, exacerbating preventable conditions.
But remember: “they” are us, and we all deserve better.
If you’re still thinking about this in terms of how we can help them by this point, stop it. That’s “patient engagement” speak, and our identify is not “patient.”
Our identity is “person,” i.e. member of the human species, class Mammalia, spending every second of life alive, for 100% of the time (until we’re not), thus making our health, and healthcare a relevant part of our lives 100% of the time. Yes, even for doctors.
We all should get a remote control.
A note ondignity: Meucci mentioned not getting the “right” treatment based on the color of your skin or the community you come from, suggesting that a smartphone could be “a great equalizer.”
That’s a powerful thought, given the indignity that confronts many Americans when they try to interface with the healthcare system at any level, including when they see their providers—whether the providers intend that or not. The hypothetical HACK app, simply by virtue of being an app, confers a sense of dignity that we might not get in the doctor’s office, or indeed anywhere else.
As a survey on dignified care put it, “Dignity is at the heart of personalization. Dignity means treating people who need care as individuals and enabling them to maintain the maximum possible level of independence, choice and control over their own lives.”
We live in an era where America’s healthcare system does not prioritize dignity. Is it possible to claw some of that back?
If you’re going to design a healthcare app to democratize healthcare access for people, that includes you.
In another Spicy Takes exchange, Stepro observes, “Isn’t it better when the consumer is educated and activated—after all, it’s our own body on the line? I’m glad folks are turning to Google or GPT for answers, even if they aren’t perfect, because it shows a healthier dynamic.” Behan responds that unvalidated or wrong information is hard to overcome, and Stepro sarcastically asks if misinformation in medicine has been a persistent issue.
Well, yeah, those problems face all of us, don’t they? We all consult with Dr. Google occasionally, because it’s free, and you can consult it at any hour and ask it any stupid question you want. The downside is that the answers aren’t reliable and can’t substitute for what an actual doctor might advise. And Dr. Google has no idea what your full medical history is (not that you want it to).
Some third-party apps like Ada Health improve dramatically on Dr. Google by using symptom checkers based on verified medical information. Chatbots based on large language models can certainly look up your ailments and dispense advice, although you should be wary if they encourage you to eat rocks. If you’re fortunate enough to have access to the Wolters Kluwer’s UptoDate clinical decision support service, you can find loads of evidence-based data refuting social misinformation. You can even get mobile access to it, and at $60 a month that’s not too shabby.
It’s still pretty far from “free,” however, and UptoDate doesn’t know whether you have a medical condition that could make any recommendations it offers highly dangerous. But if that feature is integrated into the HACK app, you lose the danger of uninformed recommendations, and get to keep the endlessly useful medical library.
On that subject, what else can we pack into this thing?
What an app wants, what an app needs
So far, the HACK app has two big features:
A library of trustworthy medical information that you can consult for any reason, at any time, that’s informed by your medical history included in the app.
Your entire medical history, including all lab results, hospital stays, specialist care, etc. regardless of which healthcare provider you saw for any of these treatments.
Let’s continue stealing important features from other smartphone apps to integrate them into the HACK app, bearing in mind that they must be for the individual using the HACK app—not features designed for providers to gather data from, or to influence the behavior of, the patients they treat.
What else?
Let’s say the app has an UptoDate level of education materials in a database that connects to your specific data and diagnosis using MedlinePlus Connect. Give the app a chatbot that can pull from this database to answer all of your questions, regardless of how sensitive or embarrassing, and deliver that information in simplified terms without jargon. Now you’ve got a semi-omniscient doctor in your pocket who can tell your uncle (or RKF Jr.) to stuff it when he goes on about vaccines causing autism.
Let’s say the app prioritizes having control over your own data and lets you update and make corrections to your EHR data using a souped-up version of OpenNotes. It also includes a data permissions management dashboard, with the ability to see an audit trail of who has accessed that information—even if there’s nothing you can do about it.
Let’s say the app can also be a buddy who just happens to have a weird fixation on making sure you follow your treatment plan. It incorporates behavior modeling tools from Health Catalyst’s UpFront app to take over remembering stuff when your brain is full (i.e., cognitive offloading). “Hey, you were supposed to schedule that colonoscopy three weeks ago—want me to go ahead and set up the appointment, ya big baby?” Okay, to be fair, Upfront would be nicer than that.
Let’s say the app can create a localized map of all healthcare providers and resources in your area that you can filter by available services. It builds this using tools like Unite Us’s resource directory or ZocDoc’s appointment booking platform, but no referrals are required—you self-refer. “Hi, I have a weird rash and need to see somebody within a week. What do you have available and how much is it going to cost?”
Let’s say the app also has a filter that flags conditions you have, and procedures you might need in the future that might become, you know, illegal in your area at some point. The app could tell you the next closest location where it’s still legal, and point to ride-sharing and other assistance to help you get there/afford it. It could even alert you to events like Texas Attorney General Ken Paxton suing HHS to slide past HIPAA protects to access data indicating you had an abortion.
For that matter, the app could shield you from (some of) the effects of federal cuts to health services with built-in compliance to existing regulatory measures that protect and preserve your data.
Let’s say the app has access to population health data showing the health risks you face most imminently and what you can do about them, incorporating those insights from Arcadia’s population health platform and Health Catalyst’s Ignite platform. The risks matter whether they’re nature or nurture, and you need to know ASAP what you can do about those affecting you.
Finally, let’s say the app, while placing all of this individualized information and these resources in a little device in your individual hand, also puts you in touch with communities of other human beings affected by the same conditions you are, by offering a feature like HealthUnlocked. You were never alone in this, and here’s the proof.
Nice little fantasy app you’ve got there. Who’s going to make it, though?
Ah, the mask has fallen. The jig is up. The cat’s out of the bag, and the deus is off the machina. What now?
Just kidding. This is a thought experiment for a reason—I don’t expect anyone to make the app. America is ripe for such an app, we need such an app, and we have the tools to create such an app—but that doesn’t mean we’re going to.
But let’s continue to be optimistic– perhaps I’m wrong on that second point. So, okay, what would developing the HACK app require?
A governing body to make sure the app is trustworthy
A sustainable funding model (Stop laughing– we just got started!)
Interoperability across all EHR vendors (I said stop laughing!)
Assume that we have satisfied all three requirements. This is, once again, a thought experiment.
Now, can we seriously address the matter of who makes the HACK app– and why?
What are our options?
The ONC
This one is obvious, because they already oversee FHIR and TEFCA, and interoperability is their dream. They also have regulatory power without a profit motive. But they don’t make software—they just regulate it. Somebody else would have to make it, and put the ONC in charge.
A private tech company (e.g. Microsoft, Google, Apple)
Microsoft attempted something similar with HealthVault, a site where users could store and share their health information, which fizzled and died in 2019.
Google Health was born in 2008, died, and then came back again, finally dying off for good in 2023.
But Apple Health is alive and kicking, using Fast Healthcare Interoperability Resources (FHIR) to let users import and view their health data on their iPhones and iPads after retrieving it. FHIR standards, importantly, were developed and adopted after Microsoft and Google made their respective shots.
When Microsoft and Google started leveraging FHIR, they were no longer in the “patient records for patients” business. Azure Health Data Services and Google Cloud Healthcare API are data platforms used by healthcare systems, payors, research institutions, and so on.
But in none of those cases was the focus on providing services based on patient records—just the records themselves. Apple Health can only function as a sort of meta-patient portal, requiring users to log into their actual patient portals to access their records, and their providers have to agree to letting Apple share the records in the first place.
If a private company like this developed the HACK app, you could argue that it democratizes access far more than the patient-portal-like products these companies previously developed, but, again—it would be their product, for better or worse, and arguably so would we.
A public-private partnership
This means:
Private tech company builds the infrastructure.
Nonprofit coalition manages the project.
ONC (or other federal agency) sets the standards and governs the data.
I guess that’s an option. But if this combination of entities could accomplish something like the HACK app today, why haven’t they done so already?
Who’s going to own it?
Taking on the project of creating the HACK app through that kind of partnership would be a tacit admission that the current system has failed, and that it’s going to take an app to save it—or at least, to survive in the face of that failure.
That’s the paradox of designing a “subversive” app promising to democratize healthcare through the backdoor, while only requiring access to all of the health records that healthcare systems are refusing to share right now, even after the ONC has hounded them to do so for over 20 years.
Each of the app’s features “stolen” from an existing technology really would have to be stolen, and it’s hard to imagine healthcare tech companies welcoming someone pirating their platforms.
On the other hand, it’s also hard to imagine a better example of the healthcare industry doing what it can to make a difference. “I helped someone understand their own medical records and make plans for future treatment today, when otherwise they wouldn’t have” is not nearly as sexy a claim as “I helped someone out of poverty today,” but it’s a lot more realistic– and on a higher scale, both of those claims could easily be true.
But because healthcare tech platforms sell patient engagement tools to providers rather than to people, there’s no motivation to develop a HACK app per se.
And even if the motivation was there, America has a population of—what—over 340 million at this point? How’s the HACK app going to reach all of us, even a large fraction of us?
How do we get this kind of reach?
Let’s assume that the HHS is developing the app—it would have to, to approach anywhere near that reach.
I’ve actually done a lot of research and writing lately about another app, developed by another U.S. federal governmental department, that reached as many as 64 million—while also stringently adhering to high security and data protection standards and relying on nationwide interoperability and data integration. It’s installed on my phone now, actually, though I’ll admit that I haven’t used it recently.
Maybe the HACK app could take some lessons from it?
Federal development and oversight—If HHS takes direct ownership of the app, just as this other agency did, that would mean developing the app in-house rather than outsourcing it to private industry.
Security and data protection—The HACK app would need to encrypt personal data, require strict user authorization as well as access control and permissions management, and comply with federal security standards, just as the other app did.
AI and automation for user navigation—Both apps rely on automated data processing, proactive notifications and engagement, AI-driven risk assessment, and smart eligibility and routing systems that guide users through decision trees based on their data.
Large-scale user support and infrastructure—Both apps must be scalable to handle millions of simultaneous users, both use mobile-first design, and both require redundancy and real-time threat monitoring for resilience against system failures and cyberattacks.
That’s a very general list of requirements, but if another government-developed app can succeed on this level, couldn’t the HACK app do the same? Assuming that the HHS has access to all information and other resources required to do it, that is.
Now, if your answer is “Yes,” how shocked will you be to learn that the other app is CBP One? You know, the app developed by Customs and Border Patrol to scan the faces of migrants and use that as a basis to determine if they can enter the country? The one that Trump shut down on his first day in office, forcing me to defend it after bashing it for months? Yes, that one.
I know, different government agency altogether. Different goals, altogether.
But that’s my point– regardless of how you think about immigration or healthcare, it says a lot that even after such an app was (successfully) developed to regulate immigration, it’s impossible to imagine the government developing a similar app to get healthcare access to Americans.
CBP One has something else in common with regular patient portal apps—it wasn’t developed for its intended end users, but rather the organizations providing the app. And as with patient portal apps, that didn’t stop government officials from boasting about how the app provides migrant empowerment—”There’s a lot of people who would love to migrate to the United States. In essence, they see CBP One as sort of a self-petitioning mechanism that we’ve never had before.”
*cough* So, anyway…
After all of this, have we democratized access to healthcare yet?
No, but we’ve shown that it’s possible to make a tool for getting there.
The U.S. in 2025 is a country:
where the best way to reach the greatest number of the population, regardless of demographics, is via a smartphone
with a disaster of a healthcare system that we have no choice but to navigate
where, within in that system, our healthcare needs are socially driven out of our hands
where huge advancements in healthcare technology have been made, and continue to be made, every day
whose government has already built a large-scale, high-security, interoperable app for mass data processing, supporting daily access by millions of people. Granted, that was for a very different purpose– but still, they did it
All of the problems standing in the way have been solved—just in different directions, for different people, with different purposes.
And now, the goddess Panacea would like a word.
She’s been quietly waiting in the wings, refusing to step anywhere near that cursed crane, even though she’s arguably the most qualified to do so.
She wants us to remember that America is now an older country than it ever has been, and older folks are sicker folks. They’re also notoriously bad with tech—but they’ve come far since the days when everybody was posting screenshots of their parents failing spectacularly at texting. And we’re at the point where the first generation to grow up using computers is eligible for AARP, anyway. So while the HACK app won’t replace their knees later on, it would be the next best thing to having a personal nurse (or tireless family member) with them 24/7.
She also points out that administrative efficiency is one of the categories included in the Commonwealth study where the U.S. tanked, with wasteful administrative spending estimated as high as $570 billion in 2019. And the HACK app could streamline patient access to records, real-time cost transparency, and insurance verification outside of the doctor’s office. Just sayin’.
Lastly, she wants us to know that the deux ex machina isn’t always what we think it is.
If your job is making boots, and you make boots for soldiers to wear to go to war, then boots are not your deus ex machina for winning the war. They’re just the tiny but significant contribution you can make, using the power and skills you have, to make winning the war more possible.
Likewise, if you’re in the business of making healthcare apps, your apps are not your deus ex machina for democratizing access to healthcare—they’re the tiny but significant contribution you can make, using the power and skills you have, to make democratized access to healthcare more possible.
She departs stage left with a warning: Stop hanging gods from cranes, she says. Just build some damn ladders, and let people climb.
In my last post (Down the patient portal: the world of healthcare tech serving you data about you) I introduced the back end of patient engagement from the patient’s perspective. While you can’t choose the digital patient engagement tools your provider uses, you can often choose your provider— and different providers may be part of different health systems, using different healthcare tech platforms and different healthcare records.
Those software platforms typically include a care management suite that integrates with the rest of apps your provider uses, but one of those apps is especially important here.
Alongside the other solutions dedicated to preventative care, patient safety, and care coordination, patient portals (under patient engagement) are the tool the provides direct access to your medical records. So I focused first on explaining EHRs and the problem of interoperability, because of the real and significant impact that these disputes, barriers, and tangles in communication have on you, the patient.
You need to know that background to understand what’s happening now, and what you can do.
Remember patient empowerment? This is it.
Looking out for yourself
If you’re lucky, you’ve never had to think about what healthcare system your doctors use. But if you’ve ever had to track down missing medical records, repeat a test you know you already did, or explain your own medication history to a doctor who should already have that information, then you’ve already felt the consequences of America’s EHR interoperability problem.
Your healthcare experience isn’t just about whether your doctor is good at their job. It’s about whether they have the right information at the right time to make the right decisions for you. If you’re bouncing between healthcare providers who use different systems, that information might not transfer correctly—or at all.
This isn’t just annoying; it’s dangerous. A lack of complete medical history can lead to misdiagnoses, medication errors, redundant tests, unnecessary procedures, and gaps in treatment. Even if you assume doctors are double-checking everything, the burden of making sure they have all your medical information often falls on you. And unless you’re carrying around a personal medical file at all times, mistakes are inevitable.
Example Scenarios:
A patient switches primary care doctors to one in a different system. The new doctor doesn’t see a past MRI that ruled out a neurological issue, so they order another scan unnecessarily.
A specialist prescribes a new medication, but the new primary care doctor can’t see it. The patient is prescribed two medications that interact poorly, leading to side effects.
A patient undergoes an outpatient procedure at a hospital in one system, then follows up with a specialist in another system. The specialist doesn’t see the records and repeats the same procedure.
While interoperability has improved in recent years, it’s still far from seamless, and you’re the one who pays the price when systems don’t communicate.
It’s not one weird trick
You might not be able to change how hospitals and EHR vendors operate, but you can make smarter choices about how you navigate the system. Here’s what you can do:
Learn which EHR system your providers use, and stick to providers within that same system when possible. If your primary care doctor, specialist, and hospital all use the same EHR, they’ll have instant access to your records instead of relying on faxes, manual transfers, or patient memory.
Use patient portals aggressively. Download your records, test results, and medication history. Keep a copy for yourself and bring it to new providers.
Request a full record transfer whenever you switch providers. Don’t assume it will happen automatically—it won’t. You’ll likely need to sign paperwork and follow up multiple times.
Know your medications and history. Keep a personal record of your prescriptions, past procedures, and major diagnoses. If a provider doesn’t have your full history, you’ll be able to fill in the gaps.
By the way– don’t confuse this with in-network vs. out-of-network
Just because a provider is “in-network” for your insurance doesn’t mean they use the same EHR system as your other doctors. You could see five in-network doctors and still have each one struggle to access the others’ records.
What does matter is whether they’re part of the same health system—a term that refers to hospital groups and affiliated practices using the same EHR. For example, a doctor at a hospital using Epic will likely have an easier time accessing records from another Epic-using provider than from one using Cerner or Meditech.
Zooming back out
Until the U.S. healthcare system makes full interoperability a reality, patients have to think strategically about where they get care. Your choice of providers can make a massive difference in the quality, efficiency, and safety of your care for reasons that go far beyond the time you spend sitting in the waiting room next to the fish tank.
And if you’ve ever thought, why isn’t there a single app where I can access all my health records in one place, no matter where I go?—you’re not the only one. That’s a problem a Healthcare Unifying Portal (HUP) app could solve, and it’s past time we had one.
Pictured: The image ChatGPT generated for this post.
The subject of patient engagement tools, especially patient portals, took up permanent residence in my head last January when my mother, a few months away from achieving octogenarian status, experienced a health event that would change both of our lives. When she came home from the hospital, suddenly she was no longer under 24-7 observation by hospital staff– she and I were on our own.
Later I learned that the hospital has a patient portal app that could help manage some of the our needs (not the personal chauffer for Mom, sadly– that was still me), and it suddenly it clicked—a mobile patient portal app could be a kind of tiny doctor that goes with you everywhere and is accessible at any time! The next thought, immediately, was “Wait, why don’t we all have that now?”
And thus began the rabbit-hole-diving—no, the portal-diving—into the research behind this post.
Patient engagement? Is that the prelude to patient marriage?
If you’re new to the idea of patient engagement in healthcare, let me break it down:
Patient engagement is the strategy of enabling patients to self-manage their healthcare needs, and patient engagement tools are online programs and services for patients to access on their own. This could include anything from tailored messages and reminders about their treatment plans and medications to educational resources to remote monitoring that tracks medication adherence.
(See also patient adherence, patient empowerment, patient autonomy, patient activation, patient experience…the terms have changed a bit over the years)
Patient portals are a patient engagement tool with a legal mandate: they are required by law to provide two services: 1) access to electronic health records (EHRs), and 2) the ability to contact and correspond with the patient’s healthcare providers. However, patient portals may also include a host of other features– and often do, because they are patient engagement tools. And they come in mobile app format, so let the features flow!
Patient engagement has potential to advance patient empowerment, which the WHO defines as “a process through which people gain greater control over decisions and actions affecting their health”—the worthiest of goals, but strangely also very distant.
Discovering why requires taking a nice long walk through the current landscape of patient engagement, stopping off to learn what EHRs even are, what healthcare tech platforms are, what the law says they have to do, and the reality of what they are doing today, before pointing out some promising possibilities sprouting up and looking hopefully into the future.
Your medical records online, no CD-ROM required
An electronic health record (EHR)1 is a digital system for storing patient health data, intended primarily for use by healthcare providers and platforms. EHRs can contain data in the following categories:
Demographic Information: Name, age, sex, race, ethnicity, and sometimes socioeconomic data like marital status or occupation.
Medical History: Diagnoses, medications, allergies, immunizations, surgeries, family history, and previous visits.
Clinical Data: Test results, imaging reports, physician notes, vital signs, and treatment plans.
Billing and Insurance: Information about coverage, claims, and payment history.
Social Determinants of Health (SDOH): The non-medical factors that impact health, such as housing status, income, education, etc.
In the context of a healthcare system like a hospital, EHR data is the central nervous system—it gets vital information in front of the people (doctors, nurses, clinicians) who need to make decisions about a patient’s care, informed by that data.
Note: When the word “patient” is used here, that’s you—provided, of course, you’ve ever sought care from a healthcare system. Keep in mind as we’re talking about who accesses EHR data and how it’s used, because that’s your data—your demographic info, your medical history, your clinical data, your billing and insurance information, and your social determinants of health (effectively, your life).
Empower Patients: Giving patients access to their health data is one of the core benefits of system interoperability. Patients are better able to seek second opinions and alternative treatments, download educational materials that can help with disease management, and access their own diagnoses and test results. They no longer need to hunt down records from multiple providers and remember when and where they sought treatment, which medications they’ve been prescribed, and the details of their treatment plans. Key to this effort is providing this comprehensive data to patients through easy-to-use applications or web pages that also include an accurate history of the data’s source.
Health records existed on paper before they were digitized, and once digitized they could be shared between healthcare systems according to the standards set in place by HIPAA, using Health Information Exchanges (HIEs)2 set up by the by the Assistant Secretary for Technology Policy and Office of the National Coordinator for Health Information Technology– the ASTP/ONC, for those of us who hate pausing to take a breath in the middle of a name.
But patients didn’t get meaningful access to their EHRs until 2014, with the implementation of the appropriately named Meaningful Use Stage 2 of the HITECH (Health Information Technology for Economic and Clinical Health) Act, proposed in 2012.
Imminent clinical information I mentioned above—diagnoses, allergies, test results, and so on—isn’t the entire set of data in an EHR, nor are clinical purposes the only reason that EHR data is accessed. The information shared via HIEs is aggregated from multiple EHRs and providers to facilitate interoperability (which we’ll get to later) and improve care coordination across systems.
Payers (insurance companies, Medicare, Medicaid) access EHR data to assess coverage, process claims, and conduct risk assessments. Public health agencies access EHR data according to health data reporting standards (including international health data reporting standards, which means the WHO, from which the U.S. is withdrawing, but not until January of 2026).
That’s a lot of entities, but a few are especially relevant here:
EHR tech platforms don’t access EHR data per se—rather, they provide EHRs for use by healthcare organizations. They’re the OG accessors, and they also provide software used to manage that data such as dashboards, reporting modules, payroll, human resources, risk management and compliance, and of course, patient engagement.
Analytics platforms don’t replace EHR platforms, so much as sit on top of them. An analytics platform integrates with the EHR platform, taking the (de-identified) data in EHRs and aggregating it, drawing insights that apply broadly and inform healthcare systems from a top-down, population-level perspective that would inform those systems at the administrative level. You can think of EHR platforms as handling healthcare in the here and now, whereas analytics platforms look toward the future.
Government and regulatory bodies that I mentioned above, including the Department Health and Human Services (HHS) division the ONC, which became the ASTP/ONC3 last July, 2024.
But The legislation with the biggest impact on patient engagement came when the ONC was still the ONC– 2016, with the 21st Century Cures Act.
The Cures Act asserted a goal of offering patients access to their electronic health information in a single, longitudinal format that is easy to understand, secure, and may be updated automatically. To support this, the act promoted the adoption of FHIR (Fast Healthcare Interoperability Resources), a modern data exchange standard that enables seamless, real-time sharing of structured health data across different systems, including EHRs, patient apps, and third-party services.
So let’s look at a few of those, already.
Gimme 5
Healthcare platforms vary wildly beyond the distinction I made between EHR and analytics platforms. In all cases, it boils down to how a platform uses EHR data—and in the case of EHR platforms, the extent to which they allow others to use that data (a big part of interoperability, which we’ll get to later).
These differences naturally determine how their patient engagement tools are going to work, so it’s necessary to take a closer look at some specific examples of those tools in the context of the entities that provide them.
For that reason I selected a sampling of five of the vendors selling those tools: a major EHR vendor, a significantly smaller EHR vendor, a platform of patient journey and educational tools, and two very different analytics vendors.
First up, let’s talk about the gorilla in the room, because he’s going to dominate a lot of the discussion that follows.
America’s biggest: Epic Systems
Epic provides a patient portal, MyChart, that links to Epic’s electronic health record (EHR) system. It’s designed for seamless patient-provider communication within the Epic ecosystem, and allows patients to view health records, schedule appointments, message providers, and manage prescriptions It was augmented recently to include telehealth integration, patient-reported outcomes tracking, and AI-driven health insights.
Messaging on Patient Engagement:
Epic markets MyChart as the gold standard in patient engagement, emphasizing its ability to enhance patient-provider communication and streamline access to records. However, its definition of interoperability is largely confined to the Epic ecosystem, making true cross-platform access challenging.
Epic’s patient engagement strategy reinforces data centralization under its platform. Its history of opposing federal interoperability mandates and allegations of information blocking combined with its public-facing support of interoperability sends slightly mixed messages.
The company has been criticized for making data sharing more difficult when external platforms (see the entry below on Particle Health) attempt to access its network.
Counterpoint: Epic’s Safety Net Initiatives
I can’t portray Epic as the all-around Big Bad when they go and do stuff like using SDoH data insights to influence policy change4 and offer Safety Net program5 tools. However, these tools don’t appear to be integrated6 into MyChart- although it does have a feature to get estimates for cost of care and what’s covered by insurance vs. self-pay. It also allows patients to “provide financial information and request assistance with paying your medical bills,” which is vague but sounds promising.
Next up is more of a refined, artisanal EHR platform that isn’t Epic’s biggest fan.7
Cloud-based EHR and practice management platform: AthenaHealth
AthenaHealth targets smaller and mid-sized healthcare providers seeking a more flexible, scalable alternative to Epic.
It’s marketed as a seamless patient experience platform, emphasizing “a connected patient experience across the care journey,” providing scheduling, secure messaging, and telehealth integration, and automated reminders and billing/payment tools to streamline administrative processes.
Messaging on Patient Engagement:
AthenaHealth positions itself as a patient-first EHR vendor, promoting “patient loyalty” as a key benefit of its engagement tools, while warning of “patient consumerism”—indicating concern over patients becoming too independent in their healthcare choices. AthenaHealth advocates for interoperability8 but has been criticized9 for remaining tied to its own system structure. While it has presented itself as more open than Epic, it still operates within its own ecosystem, limiting cross-platform functionality.
Moving on from EHRs, the next stop is a school for patients.
Clinical decision support (CDS) and patient education: Wolters Kluwer
Wolters Kluwer Health is expanding into patient education and engagement through digital tools.
UpToDate10 is a suite of clinical decision support (CDS) tools for providers, with patient education resources tailored to treatment plans and AI-powered patient journey tools that offer personalized treatment explanations by integrating into EHRs.11
Messaging on Patient Engagement:
UpToDate is marketed as a trustworthy, evidence-based resource for both providers and patients. Unlike Epic or AthenaHealth, Wolters Kluwer’s approach to engagement is more about education than direct patient interaction.
Wolters Kluwer emphasizes its role in enhancing shared decision-making by ensuring patients and clinicians have access to the same information. They have also been a strong advocate for patient empowerment. Their messaging emphasizes the need for better tools, education, and data access to facilitate truly patient-centered care.
Counterpoint: Wolters Kluwer’s positioning on patient empowerment varies, depending on whether they’re talking to healthcare systems or sharing the perspective of one doctor12 advocating for patient empowerment.
Their white paper on the “patient empowerment framework”13 includes this curious statement:
There are many aspects to patient empowerment, but in general, understanding of this concept is fragmented. There are not agreed-upon definitions for terms like activation or engagement. And there is no comprehensive understanding of how these various aspects fit together.
So…I guess we can just define these terms however we want? Because UptoDate referencing how “patient empowerment is a critical component to operating profitability in this new world” doesn’t sound so much like patient empowerment to me, as a money-making strategy. Not that turning a profit is a bad thing, but can we have one term that’s about patients, not turning them into products?
I suspect that this first analytics platform won’t have an answer, but nobody’s perfect– especially this one.
Data Aggregation and Patient Analytics: Particle Health
Particle’s engagement tools include data retrieval services that allow providers to query national HIEs, and a Record Locator Service (RLS) that predicts where patients have received care based on historical data.
Messaging on Patient Engagement:
Particle Health promotes its Record Locator Service (RLS)14 as a way to track patient’s movements between healthcare providers, even promising giving clients a notification “when a patient receives a high-value procedure out of network,” so that they can “ensure high-value procedures are scheduled in-network.”
In addition to making the words “patient journey” in its mission statement: “Drive strategic growth with patient journey insights” sound rather ominous, this level of patient tracking sounds like more of a patient stalking tool than just an engagement platform. Interoperability is one thing, but sharing real-time insights into where patients have been just feels like it’s crossing a line.
Counterpoint: Particle does get credit for its challenge to information-blocking on the part of Epic, filing a federal antitrust lawsuit15 alleging that Epic used its dominance in the EHR market to cut off its own customers from being able to request data from Particle, impacting over 420,000 patients—they even created a dashboard16 showing which organizations were involved. I believe the suit is still ongoing, so it’s something to watch.
But for now, maybe there’s an analytics platform less inclined to follow you down dark alleys.
UpFront’s predictive analytics bring healthcare closer to the ideal of proactive, personalized care.
It uses psychographic segmentation and behavior modeling to influence patient choices:
AI-driven outreach for scheduling, reminders, and follow-ups
Segmentation of patients based on psychological and social factors
Categorizes patients based on real-time risk factors, including SDoH data
Proactively reaches out to high-risk patients before their conditions worsen
Adjusts outreach based on a patient’s engagement level, ensuring personalized interaction
Helps providers optimize follow-ups and interventions based on patient responses and historical data
Messaging on Patient Engagement:
UpFront promotes psychographic segmentation18 as “hyper-personalized patient engagement,” claiming to improve patient follow-through by understanding motivational drivers. It frames its AI-powered approach to increase patient activation and reduce provider workload.
One potential benefit of psychographic segmentation: personalized patient engagement: by understanding patients’ attitudes, values, and lifestyles, healthcare providers can tailor communications and interventions to better align with individual motivations, potentially leading to improved health outcomes.
Counterpoint: There are, however, prominent criticisms of psychographic segmentation, such as:
Privacy Concerns:19 There are concerns about the ethical implications of collecting and utilizing detailed personal data for segmentation, including potential breaches of patient privacy and the risk of manipulating patient behavior without informed consent.
Data profiling: Concerns about how patient behaviors are categorized and acted upon. Its focus on steering patients toward “desired actions” can blur the line between engagement and subtle coercion.
Risk of Overgeneralization:20 Assigning patients to broad psychographic categories may overlook individual nuances, leading to interventions that fail to address specific patient needs or circumstances.
If UpFront wants to be your health coach, Health Catalyst’s other patient engagement app is more about being your personal health assistant.
Automated patient engagement and communication platform: Twistle
Twistle improves adherence by meeting patients where they are—through familiar communication channels.
It takes the manual burden off healthcare providers by sending reminders, check-ins, and education materials to patients, using their EHR data and self-reported responses to adjust engagement over time. Other features:
Sends automated reminders for medication adherence, upcoming appointments, and follow-up care, that uses multi-channel automated messaging (text, email, phone, app notifications)
Uses secure messaging to check in with patients post-discharge
Integrates with wearables and home monitoring devices, pulling in real-time patient data for more personalized outreach
Uses SDoH data to adjust engagement—patients flagged as high-risk due to economic instability
Care pathway guidance, helping patients stay on track with their treatment
Messaging on Patient Engagement
Twistle aims to reduce provider workload through automated patient communication and help patients follow their care plans with automated messaging.
A real-world case study21 focuses on Providence Health’s effort to simplify treatment for total joint replacement care, showcasing how Twistle’s automated communication and reminders reduced complications and improved patient adherence to pre- and post-operative care plans. Twistle emphasizes that its platform allows for seamless digital engagement, helping patients stay informed and compliant with their treatment, ultimately leading to better outcomes and cost reductions.
While all of these platforms access and use EHR data, their levels of access to it vary. Interoperability means cooperation, and some kids want to take their ball and go home.
Lack of interoperability: A fancy term for “Why can’t my doctor see my records?”
Information blocking, the art of making data hard to share22
Information blocking in healthcare refers to practices that unreasonably prevent or limit the sharing, access, or use of electronic health information (EHI) among patients, providers, or health systems, often for competitive or financial reasons.
Sharing data between different health systems is what determines how useful patient engagement tools can be. The ability of different healthcare information systems and applications to access, exchange, integrate, and cooperatively use data in a coordinated manner across organizational, regional, and national boundaries ensures that patient information can be shared seamlessly among providers, labs, pharmacies, and other stakeholders to improve care quality, efficiency, and patient outcomes.
The 21st Century Cures Act and HTI-1 Final Rule were supposed to stop hospitals and EHR vendors from blocking access to patient data. But instead of embracing real interoperability, vendors found loopholes, such as:
Charging high fees for data access, making it financially unfeasible for competitors to build better patient engagement tools
Requiring custom-built API integrations for every new connection, forcing external developers to spend months negotiating and developing integrations that should be standardized.
Allowing hospitals to delay lab result releases until after a doctor manually reviews them, even if laws require immediate electronic availability
Internal interoperability works great—within that hospital system. But if a patient moves to another provider? Suddenly, data transfer becomes a bureaucratic mess. For example:
Vendor lock-in/EHR monopoly
Epic, Oracle (Cerner), and Meditech together control 60% of U.S. hospital EHRs. If a hospital uses Epic, it uses MyChart. If it uses Oracle, it’s HealtheLife. If it’s on Meditech, it’s Meditech Expanse.
Interoperability between different EHR systems remains limited, often resulting in hospitals remaining dependent on their existing systems. Contributing factors include:
Lack of Standardization: The absence of uniform standards across EHR systems leads to inconsistent data formats and communication challenges, hindering seamless data exchange.
Technical Complexity: The use of multiple incompatible EHR systems creates data silos and causes duplication of patient records, some of which are incomplete or inaccurate.
Patient engagement as a retention tool
To be fair, it’s just a fact that EHRs were developed for providers, not patients. That doesn’t seem quite as weird if you start with the idea that when EHR adoption surged due to HITECH Act incentives (2009-2015), vendors focused on first on helping hospitals meet Meaningful Use requirements (i.e., digitizing patient records and improving provider efficiency).
The primary customers for EHR systems are hospitals, not patients, so vendors designed tools that optimized billing, scheduling, and regulatory compliance rather than patient-facing features. Insofar as they thought about patient portals, they were just minimal add-ons, basic tools.
But here’s where I stop being fair. Next, hospitals began buying third-party engagement tools to supplement clunky EHR portals, signaling that EHR vendors were failing to meet patient expectations. Rather than improve interoperability, EHR vendors responded by building their own engagement tools, and now we have competition– to best serve the needs of hospitals, that is, not patients.
Learning more about EHRs, and EHR providers specifically, caused me to recall that scene in Miracle on 34th street (my mother’s favorite movie) where Kris Kringle (aka Santa Claus) is working at Macy’s, listening to children’s wishes, when a woman asks him where to find a particular item that Macy’s doesn’t carry, distraught because the item will be a Christmas gift for her son. Kris informs her about another, competing store where she can find the gift.
This causes department head, Mr. Shellhammer, to become incensed—until he receives a deluge of letters and phone calls from customers saying how much they appreciate the Macy’s priority of helping customers over direct profit. Mr. Shellhammer immediately instructs all sales assistants to follow Kris’s lead.
But in this case, EHR Macy’s actually makes the gift, and the other stores all make their own versions of the gift, and there’s not a lot Mr. ONC Shellhammer—or Mrs. Healthcare Provider, the customer—can do about it. She can shop at Macy’s or another store, but she has a contract with Macy’s (or something—stick with me here) to buy their gifts, so it’s extremely difficult to go to another store. And her Patient son gets (almost) no say in the matter.
Okay, so it’s not a perfect analogy—we left out the parts that weren’t in the original story, such as the gift expert analysts who go around telling stores how their gifts could work better, but who also make their own gifts.
Analytics platforms: using AI to give your EHR a workout
While EHR vendors continue to dominate patient engagement through their own proprietary tools, analytics platforms are emerging as a workaround, leveraging interoperability and AI to provide a more holistic, patient-centered approach to engagement. These platforms are built to ingest, analyze, and act on patient data across multiple sources, rather than restricting data within a single EHR ecosystem.
Analytics platforms are leveraging AI to go beyond simple patient record management and actively shape engagement strategies based on real-time data, predictive modeling, and personalized interventions. These tools are helping shift patient engagement from a reactive process (waiting for patients to seek care) to a proactive model that anticipates needs and removes barriers to access.
Breaking Down EHR Silos (Health Catalyst, Arcadia) – AI-driven analytics platforms integrate data from multiple EHRs, insurance claims, HIEs, and even social determinants of health (SDoH) sources to create a comprehensive patient profile that traditional EHR patient portals cannot provide.
Predictive Modeling for Preventive Care (Arcadia, Health Catalyst) – AI-driven platforms assess millions of data points to identify high-risk patients before they require costly interventions, enabling earlier engagement and better outcomes.
Automated Patient Navigation and Outreach (UpFront, Twistle by Health Catalyst) – AI-enhanced platforms analyze patient history, social determinants, and engagement patterns to determine the most effective outreach method—whether it’s text reminders, digital education, or community resource referrals.
AI-Driven Virtual Care Coordination (Wolters Kluwer, IBM Watson Health) – AI can recommend follow-up appointments, coordinate referrals between specialists, and track adherence to care plans without requiring constant human oversight.
Real-Time Insights for Patient Adherence (Twistle by Health Catalyst, Wellframe) – AI can monitor which patients are engaging with their care plans, flagging those at risk of non-adherence and providing tailored interventions to improve compliance.
Bias Detection and Personalized Equity Adjustments (Epic SDoH Analytics, Google Health AI) – AI models can analyze how different populations receive care, identifying disparities and ensuring more equitable engagement strategies tailored to historically underserved communities.
Don’t hold back: moving beyond EHR-restricted patient engagement
As analytics platforms continue to expand their capabilities, they challenge the traditional role of EHR vendors in controlling patient engagement. While EHRs will always be necessary for core medical documentation, their ability to drive meaningful, proactive engagement remains limited. Analytics platforms are filling that gap by:
Enhancing interoperability to create unified, patient-centered data systems.
Using AI-driven insights to tailor engagement at the individual level.
Expanding patient access beyond clinical settings, incorporating SDoH and predictive health modeling.
By shifting the focus from reactive EHR-based portals to proactive analytics-driven engagement, these platforms are redefining how and when patients interact with their health data—offering a glimpse at what true patient empowerment could look like.
P.S. Oh yeah, remember that gift from Macy’s?
Turns out that the gift Ms. Healthcare Provider was trying to buy was a biography about the boy, and one that he, himself, was only recently allowed to read.
But read it he did, and the knowledge empowered him to write his own book– an autobiography, this time.
Dear reader– in a stunning twist you never saw coming, that little boy is you.
Biography or autobiography, people are going to keep copying sections of it for different purposes. But it’s still yours.
Get it, Check it, Use it! Easy access to your health records puts you in control of decisions regarding your health and well-being.
In the end, we must turn away from the abstract and distant disputes between entities who have no idea who we are, and yet handle our personal information daily. It will probably always feel like an invasion of privacy, no matter how many safeguards are in place. Equally, at some point we have to reckon with the fact that we don’t choose the patient engagement tools we use—Mrs. Healthcare Provider does, so that’s why Macy’s caters to her, not us.
But you know what? We do get to look at what we’ve been given and decide that it’s not good enough, and some of those folks are listening. So my next post will be much less structured and much shorter (it had better be!), but much louder. I plan to yell about some things– perhaps you’ll join me?